Book an Appointment
Hyperprolactinemia

Hyperprolactinemia
HYPERPROLACTINEMIA
- Prolactin(PRL) is a single-chain peptide hormone secreted from lactotroph cells of the anterior pituitary gland.
- Prolactin exerts its main physiological role by promoting milk secretion of mammary glands during the postpartum period.
PROLACTIN SERUM ISOFORMS
Prolactin exists in three major circulating molecular isoforms.
- Monomeric or little PRL (molecular weight [MW] 23 kDa) - the major circulatory isoform (80–95%) of the total prolactin in healthy subjects and those with prolactinomas.
- Dimeric or big PRL (MW 45–60 kDa)
- Multimeric / big-big PRL or macro prolactin ( MW> 150 kDa)
Dimeric and Multimeric correspond to less than 10% of the total PRL (1).
PROLACTIN SECRETION
- Prolactin secretion is pulsatile and follows a circadian rhythm with the highest plasma concentration reached during sleep, and the lowest observed in the morning about 2–3h after waking up (2).
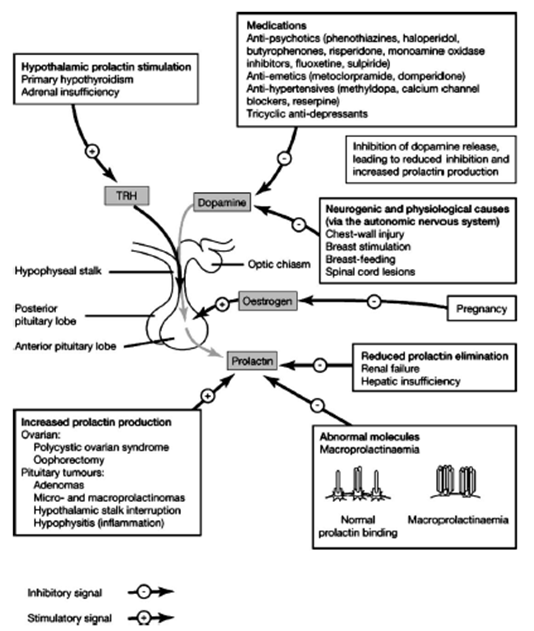
Fig. 1. Prolactin secretion(3).
NOTE -The predominant regulatory signal is the inhibition of prolactin secretion by the neurotransmitter, dopamine, from neurons in the hypothalamus (2).
HYPERPROLACTINEMIA
- Hyperprolactinemia is defined as the presence of abnormally high levels of prolactin in the blood above normal levels 0f 10–28 mg/L in women and 5–10 mg/L in men.
PREVALENCE
- The prevalence of hyperprolactinemia ranges from 0.4% in an unselected adult population to as high as 9-17% in women with reproductive diseases.
CLINICAL SIGNS AND SYMPTOMS
- It is present in 10% to 25% of women with secondary amenorrhea or oligomenorrhea, in 30% of women with galactorrhea or infertility, and in 75% of those with both amenorrhea and galactorrhea (4).
- Hyperprolactinemia causes hypogonadotropic hypogonadism (HH) which is due to suppression of pulsatile GnRH thus causing anovulation, hypoestrogenism, and thus osteoporosis in perimenopausal women.
- When hyperprolactinemia is caused by a prolactinoma, additional pressure symptoms may include headaches, visual field defects, and abnormal pituitary function.
- Hyperprolactinemia in men may result in decreased libido, impotence, decreased sperm production, infertility, weight gain, and osteoporosis [4]
ETIOLOGY
Potential causes of hyperprolactinemia are listed in the table 1below .(5)
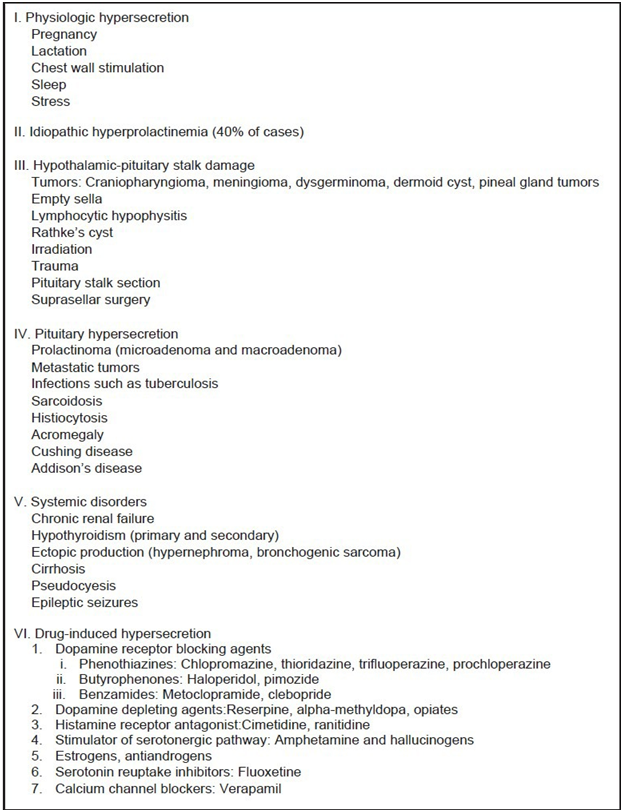
- The most frequent cause of persistent hyperprolactinemia is the presence of a micro- (<10 mm diameter) or macroprolactinoma(>10 mm). These pituitary tumors either may produce an excessive amount of prolactin or disrupt the normal delivery of dopamine from the hypothalamus to the pituitary. Raised prolactin levels can also be caused by pituitary adenomas consecrating prolactin hormone. (4)
- Idiopathic hyperprolactinemia accounts for 30–40% of cases where there is no obvious cause for the disorder and hypothalamic-pituitary anatomy is normal. (4)
- Macroprolactinemia–It's a condition where more than 60% of circulating PRL is made up of macroprolactin, which has low biologic activity instead of the normal 5-10%. Hyperprolactinemia related to macroprolactin is due to its lower renal clearance, longer half-life, and its lower capability to activate hypothalamic dopaminergic tone, which negatively regulates the secretion of pituitary prolactin(6). These patients are usually asymptomatic and no medication or further tests are recommended.
DIAGNOSIS
- Exclude physiological and pharmacological causes on history.
- Evaluate signs of hypothyroidism, hypogonadism, renal failure, and visual field defects.
- Measure S. Prolactin. Also measure TSH, free T4, and creatinine levels to rule out primary hypothyroidism and renal failure (7)
- PRL levels greater than 500 mg/l are commonly seen in macroprolactinoma. PRL levels> 250mg/l usually indicate the presence of a prolactinoma; however, prolactinoma cannot be excluded in the presence of lower levels, and PRL levels >100mg/l are present in some patients with idiopathic hyperprolactinemia. Several drugs may cause PRL elevations above 200 mg/l (8 ).
- Hyperprolactinemia without an identified cause requires imaging of the hypothalamic-pituitary area. Although Computerized axial tomography (CAT) scan can be used, a magnetic resonance image (MRI) with gadolinium enhancement provides the best visualization of the sellar area. (8)
Endocrine Society Clinical Practice Guidelines for Diagnosis (9).
- To establish the diagnosis of hyperprolactinemia, a single measurement of fasting serum prolactin is recommended(2-3 hrs after waking up ); a level above the upper limit of normal confirms the diagnosis as long as the serum sample was obtained without excessive venipuncture stress. Dynamic testing of prolactin secretion for the diagnosis of hyperprolactinemia is not recommended (1 )
- In patients with asymptomatic hyperprolactinemia, the screening of macroprolactinomas is recommended by polyethyleneglycol- (PEG-) precipitation method and the confirmative and qualitative examinations include gel chromatography, protein A/G column and 125I-PRL binding studies (6)(2|).
- When there is a discrepancy between a very large pituitary tumor and a mildly elevated prolactin level, do serial dilution of serum samples to eliminate an artifact that can occur with some immune radiometric assays leading to a falsely low prolactin value (“hook effect”) (1| ).
TREATMENT :
Endocrine Society Clinical Practice Guideline for Management of drug-induced hyperprolactinemia (9).
- Exclude medication use, renal failure, hypothyroidism, and para-sellar tumors in patients with symptomatic non-physiological hyperprolactinemia (1| ).
- In a symptomatic patient with suspected drug-induced hyperprolactinemia, discontinue the medication for 3 days or substitute an alternative drug, followed by remeasurement of serum prolactin(2|).
- If the drug cannot be discontinued and the onset of the hyperprolactinemia does not coincide with therapy initiation, do a pituitary magnetic resonance image (MRI) to differentiate between medication-induced hyperprolactinemia and symptomatic hyperprolactinemia due to a pituitary or hypothalamic mass (1|).
- Do not treat patients with symptomatic medication-induced hyperprolactinemia(2|).
- Use estrogen or testosterone in patients with long-term hypogonadism (hypogonadal symptoms or low bone mass) related to medication-induced hyperprolactinemia(2|ÅOOO).
TREATMENT OF PROLACTINOMAS – Dopamine agonists are the drug of choice.
Table 2. Comparison between Bromocriptine and Cabergoline in the treatment of hyperprolactinemia (10).
|
|
Bromocriptine |
Cabergoline |
|
Dopamine receptor target sites |
D1 and D2 |
D1 (low affinity) and D2 (high affinity) |
|
Duration of action |
8–12 h |
7–14 days |
|
Half-life (h) |
3.3 |
65 |
|
Available doses |
1.0 and 2.5 mg scored tablets; 5 and 10 mg capsules |
0.5 mg scored tablets |
|
Typical dose |
2.5 mg/day in divided doses |
0.5 mg/week or twice-weekly |
|
Dosing regimens, starter packs, dosage |
Start on 1.25–2.5 mg/day at bedtime. Gradually increase to a median of 5.0–7.5 mg/day and a maximum of 15–20 mg/day |
Start at 0.25–0.5 mg twice weekly. Adjust by every 2–4 months according to serum prolactin levels |
|
Advantages |
A long history of use; does not appear to be teratogenic; inexpensive |
Good efficacy; low frequency of adverse events; may be useful in bromocriptine-resistant patients; weekly or twice-weekly dose |
|
Disadvantages |
Tolerance; recurrence; resistance; multiple daily dosing |
Not yet indicated for use during pregnancy |
|
Common side effects |
Nausea, headache, dizziness, abdominal pain, syncope, orthostatic hypotension, fatigue |
Milder and less frequent compared with bromocriptine |
Endocrine Society Clinical Practice Guideline for Management of Prolactinoma (9).
- Use dopamine agonist therapy to lower prolactin levels, decrease tumor size, and restore gonadal function for patients harboring symptomatic prolactin-secreting microadenomas or macroadenomas( 1|).
- Cabergoline is preferred to other dopamine agonists because it has higher efficacy in normalizing prolactin levels, as well as a higher frequency of pituitary tumor shrinkage( 1|).
- Do not treat asymptomatic patients harboring micro prolactinomas with dopamine agonists(2|).
- Treat with dopamine agonist or oral contraceptive in patients with amenorrhea caused by a microadenoma(2|).
- With careful clinical and biochemical follow-up, therapy may be tapered and perhaps discontinued in patients who have been treated with dopamine agonists for at least 2 yr, who no longer have elevated serum prolactin, and who have no visible tumor remnant on MRI(2|).
Endocrine Society Clinical Practice Guideline for ManagementofResistant and malignant prolactinoma (9)
- For symptomatic patients who do not achieve normal prolactin levels or show a significant reduction in tumor size on standard doses of a dopamine agonist, increase the dose to maximal tolerable doses before referring the patient for surgery ( 1|).
- Patients who are resistant to bromocriptine be switched to cabergoline( 1|).
- Trans-sphenoidal surgical resection of the prolactinoma remains the main option for patients who may refuse or do not respond to long-term pharmacological therapy (2|ÅOOO)
- Radiotherapy and/or estrogens are also reasonable choices if surgery fails. (2|)
- Chemotherapy with temozolomide is limited to resistant and malignant prolactinomas (2|)
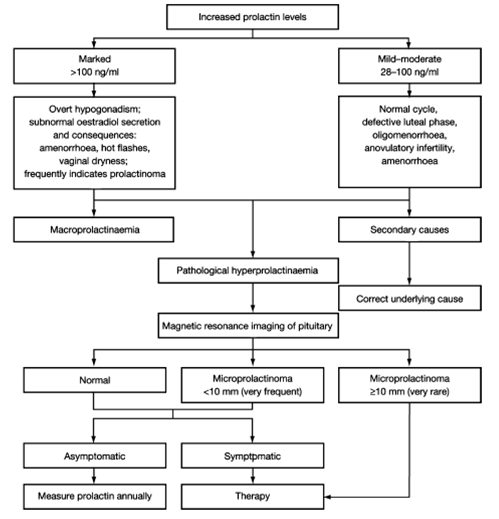
Fig. 2 -Management of Hyperprolactinoma (3)
MANAGEMENT OF PROLACTINOMAS DURING PREGNANCY
During normal pregnancy, serum prolactin rises progressively to around 200-500 ng/mL.
The Endocrine Society clinical guidelines for the diagnosis and treatment of hyperprolactinemia during pregnancy (9)
- Women with prolactinomas are instructed to discontinue dopamine agonist therapy as soon as they discover that they are pregnant(1|).
- . In selected patients with macroadenomas who became pregnant on dopaminergic therapy and who have not had prior surgical or radiation therapy, it may be prudent to continue dopaminergic therapy throughout the pregnancy, especially if the tumor is invasive or is abutting the optic chiasm(1|).
- In pregnant patients with prolactinomas, do not perform serum prolactin measurements during pregnancy (1| ).
- Pituitary MRI during pregnancy in patients with microadenomas or intrasellar macroadenomas is not recommended unless there is clinical evidence of tumor growth such as visual field compromise (1|).
- Women with macroprolactinomas who do not experience pituitary tumor shrinkage during dopamine agonist therapy or who cannot tolerate bromocriptine or cabergoline be counseled regarding the potential benefits of surgical resection before attempting pregnancy(1|).
- Visual field assessment followed by MRI without gadolinium in pregnant women with prolactinomas is recommended who experience severe headaches and/or visual field changes(1|).
- Bromocriptine therapy is recommended in patients who experience symptomatic growth of a prolactinoma during pregnancy s(1|)
CONCLUSIONS
- Hyperprolactinemia is a common pituitary hormone disorder usually found in both sexes with abnormal sexual and/or reproductive function or with galactorrhea.
- Asymptomatic patients with microprolactinemia do not require any treatment.
- Cabergoline is the drug of choice, however, in pregnancy, Bromocriptine is preferred.
- Persistent Hyperprolactinemia without an identified cause requires imaging of the hypothalamic-pituitary area.
- Giant or aggressive prolactinomas may require multiple approaches involving surgery, radiotherapy, or both.
Get In Touch
Tags
- Dr. Shalini Gynaecologist
- Dr. Shalini Gynaecologist alaknanda
- Dr. Shalini Chawla Gynaecologist
- Dr. Shalini Chawla Saket
- Best ivf centre in saket
- Best IVF Centre in Saket
- Best Infertility treatment in Saket
- Best IUI Centre in Saket
- Best IVF Centre in Saket
- best ICSI centre in Saket
- Best Fertility Doctor in Saket
- Best IVF Doctor in Saket
- Low cost IVF Centre in Saket
- ovulation Induction Treatment in Saket
- Best Embryo transfer Centre in Saket
- Best Blastocyst Transfer Centre in Saket
- Best Female infertility treatment in Saket
- Best Male infertility treatment in Saket
- Blocked Fallopian Tubes treatment in Saket
- Best PCOS treatment in Saket
- Best PCOD treatment in Saket
- Polycystic ovaries treatment in Saket
- Best Endometriosis Treatment in Saket
- unexplained Infertility treatment in Saket
- Low AMH in Saket
- Poor ovarian reserve treatment in Saket
- Poor responder treatment in Saket
- Fibroid Uterus treatment in Saket
- Myoma in Saket
- Endometrial Polyp Treatment in Saket
- Hysteroscopy Polypectomy Treatment in Saket
- Hysteroscopy septum resection Treatment in Saket
- Recurrent Implantation Failure treatment in Saket
- Repeated IVF Failure treatment in Saket
- PGD Treatment in Saket
- PGS Treatment in Saket
- Best Oncofertility treatment in Saket
- Oocyte Freezing treatment in Saket
- Adenomyosis treatment in Saket
- Best infertility Doctor in Saket
- Best IVF results in saket
- Best IVF success rate in Saket
- Best IUI results in saket
- Best IUI success rate in saket
- Best ICSI centre in saket
- Low cost IUI in saket
- clomiphene citrate in saket
- Letrozole in saket
- Donor egg cycle in saket
- Donor IVF in saket
- Low sperm count in saket
- Azoospermia in saket
- Treatment of Azoospermia in saket
- Testicular sperm extraction in saket
- micro testicular sperm extraction in saket
- TESA in saket
- TESE in saket
- PESA in saket
- Microtese in saket
- surgical sperm retrieval in saket
- Donor sperm IUI in saket
- Fibroid uterus in saket
- Myomectomy in saket
- Laparoscopy in saket
- Laparoscopy for Fallopian tube testing in saket
- Advanced Laparoscopy in infertility in saket
- Diagnostic Laparoscopy in infertility in saket
- Hydrosalpinx treatment in saket
- Laparoscopy for Hydrosalpinx in saket
- Hydrosalpinx in infertility in saket
- Laparoscopy for unexplained infertility in saket
- Laparoscopy for endometriosis in saket
- Endometriotic cyst removal in saket
- ovarian cyst in saket
- Laparoscopic cyst removal in saket
- Hydrosalpinx tubal clipping in saket
- Hydrosalpinx salpingectomy in saket
- ovarian drilling in saket
- laparoscopic ovarian drilling in saket
- Hysteroscopy in infertility in saket
- pre- IVF Hysteroscopy in saket
- Diagnostic Hysteroscopy in saket
- Operative Hysteroscopy in saket
- Adhesiolysis Hysteroscopy in saket
- synechiolysis in Hysteroscopy in saket
- synechiae in saket
- PGT in saket
- Embryo freezing in saket
- Frozen Embryo transfer in saket
- Fresh embryo transfer in saket
- Day 3 embryo transfer in saket
- Assissted laser hatching in IVF in saket
- Laser hatching in embryo transfer in saket
- tuberculosis in infertility in IVF
- Blocked Fallopian tubes in saket
- egg freezing in saket
- embryo freezing in saket
- Antagoist protocol in IVF in saket
- Long protocol in IVF in saket
- Dual stimulation in IVF in saket
- Laparoscopy hysterectomy in saket
- uterus removal in saket
- laparoscopic uterus removal in saket
- adenomyomectomy in saket
- Adenomyoma in IVF in saket
- Mirena insertion in saket
- Irregular periods in saket
- abnormal uterine bleeding in saket
- dysfunctional uterine bleeding in saket
- Normal Delivery in saket
- Low Cost Delivery in saket
- Caesarian in saket
- LSCS in saket
- Low cost LSCS in saket
- Low cost caesarian in saket
- Treatment of recurrent abortion in saket
- repeated abortion in saket
- Thin Endometrium in saket
- asherman’s syndrome in saket
- ERA in saket
- endometrial receptive array in saket
- Best ivf centre in Kalkaji
- Best IVF Centre in Kalkaji
- Best Infertility treatment in Kalkaji
- Best IUI Centre in Kalkaji
- Best IVF Centre in Kalkaji
- best ICSI centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Best IVF Doctor in Kalkaji
- Low cost IVF Centre in Kalkaji
- ovulation Induction Treatment in Kalkaji
- Best Embryo transfer Centre in Kalkaji
- Best Blastocyst Transfer Centre in Kalkaji
- Best Female infertility treatment in Kalkaji
- Best Male infertility treatment in Kalkaji
- Blocked Fallopian Tubes treatment in Kalkaji
- Best PCOS treatment in Kalkaji
- Best PCOD treatment in Kalkaji
- Polycystic ovaries treatment in Kalkaji
- Best Endometriosis Treatment in Kalkaji
- unexplained Infertility treatment in Kalkaji
- Low AMH in Kalkaji
- Poor ovarian reserve treatment in Kalkaji
- Poor responder treatment in Kalkaji
- Fibroid Uterus treatment in Kalkaji
- Myoma in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Hysteroscopy Polypectomy Treatment in Kalkaji
- Hysteroscopy septum resection Treatment in Kalkaji
- Recurrent Implantation Failure treatment in Kalkaji
- Repeated IVF Failure treatment in Kalkaji
- PGD Treatment in Kalkaji
- PGS Treatment in Kalkaji
- Best Oncofertility treatment in Kalkaji
- Oocyte Freezing treatment in Kalkaji
- Adenomyosis treatment in Kalkaji
- Best ivf centre in CR Park
- Best IVF Centre in CR Park
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- Best IVF Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Best Male infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best PCOS treatment in CR Park
- Best PCOD treatment in CR Park
- Polycystic ovaries treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- Recurrent Implantation Failure treatment in CR Park
- Repeated IVF Failure treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best ivf centre in Nehru Place
- Best IVF Centre in Nehru Place
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- Best IVF Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Best Male infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best PCOS treatment in Nehru Place
- Best PCOD treatment in Nehru Place
- Polycystic ovaries treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- Recurrent Implantation Failure treatment in Nehru Place
- Repeated IVF Failure treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best ivf centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Best Male infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best PCOS treatment in Greater Kailash
- Best PCOD treatment in Greater Kailash
- Polycystic ovaries treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- Recurrent Implantation Failure treatment in Greater Kailash
- Repeated IVF Failure treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best ivf centre in South Delhi
- Best IVF Centre in South Delhi
- Best Infertility treatment in South Delhi
- Best IUI Centre in South Delhi
- Best IVF Centre in South Delhi
- best ICSI centre in South Delhi
- Best Fertility Doctor in South Delhi
- Best IVF Doctor in South Delhi
- Low cost IVF Centre in South Delhi
- ovulation Induction Treatment in South Delhi
- Best Embryo transfer Centre in South Delhi
- Best Blastocyst Transfer Centre in South Delhi
- Best Female infertility treatment in South Delhi
- Best Male infertility treatment in South Delhi
- Blocked Fallopian Tubes treatment in South Delhi
- Best PCOS treatment in South Delhi
- Best PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Best Endometriosis Treatment in South Delhi
- unexplained Infertility treatment in South Delhi
- Low AMH in South Delhi
- Poor ovarian reserve treatment in South Delhi
- Poor responder treatment in South Delhi
- Fibroid Uterus treatment in South Delhi
- Myoma in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Hysteroscopy Polypectomy Treatment in South Delhi
- Hysteroscopy septum resection Treatment in South Delhi
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD Treatment in South Delhi
- PGS Treatment in South Delhi
- Best Oncofertility treatment in South Delhi
- Oocyte Freezing treatment in South Delhi
- Adenomyosis treatment in South Delhi
- Best ivf centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- Best Infertility treatment in Malviya Nagar
- Best IUI Centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- best ICSI centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Best IVF Doctor in Malviya Nagar
- Low cost IVF Centre in Malviya Nagar
- ovulation Induction Treatment in Malviya Nagar
- Best Embryo transfer Centre in Malviya Nagar
- Best Blastocyst Transfer Centre in Malviya Nagar
- Best Female infertility treatment in Malviya Nagar
- Best Male infertility treatment in Malviya Nagar
- Blocked Fallopian Tubes treatment in Malviya Nagar
- Best PCOS treatment in Malviya Nagar
- Best PCOD treatment in Malviya Nagar
- Polycystic ovaries treatment in Malviya Nagar
- Best Endometriosis Treatment in Malviya Nagar
- unexplained Infertility treatment in Malviya Nagar
- Low AMH in Malviya Nagar
- Poor ovarian reserve treatment in Malviya Nagar
- Poor responder treatment in Malviya Nagar
- Fibroid Uterus treatment in Malviya Nagar
- Myoma in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Hysteroscopy Polypectomy Treatment in Malviya Nagar
- Hysteroscopy septum resection Treatment in Malviya Nagar
- Recurrent Implantation Failure treatment in Malviya Nagar
- Repeated IVF Failure treatment in Malviya Nagar
- PGD Treatment in Malviya Nagar
- PGS Treatment in Malviya Nagar
- Best Oncofertility treatment in Malviya Nagar
- Oocyte Freezing treatment in Malviya Nagar
- Adenomyosis treatment in Malviya Nagar
- Best ivf centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- Best Infertility treatment in Vasant Kunj
- Best IUI Centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- best ICSI centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Best IVF Doctor in Vasant Kunj
- Low cost IVF Centre in Vasant Kunj
- ovulation Induction Treatment in Vasant Kunj
- Best Embryo transfer Centre in Vasant Kunj
- Best Blastocyst Transfer Centre in Vasant Kunj
- Best Female infertility treatment in Vasant Kunj
- Best Male infertility treatment in Vasant Kunj
- Blocked Fallopian Tubes treatment in Vasant Kunj
- Best PCOS treatment in Vasant Kunj
- Best PCOD treatment in Vasant Kunj
- Polycystic ovaries treatment in Vasant Kunj
- Best Endometriosis Treatment in Vasant Kunj
- unexplained Infertility treatment in Vasant Kunj
- Low AMH in Vasant Kunj
- Poor ovarian reserve treatment in Vasant Kunj
- Poor responder treatment in Vasant Kunj
- Fibroid Uterus treatment in Vasant Kunj
- Myoma in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Hysteroscopy Polypectomy Treatment in Vasant Kunj
- Hysteroscopy septum resection Treatment in Vasant Kunj
- Recurrent Implantation Failure treatment in Vasant Kunj
- Repeated IVF Failure treatment in Vasant Kunj
- PGD Treatment in Vasant Kunj
- PGS Treatment in Vasant Kunj
- Best Oncofertility treatment in Vasant Kunj
- Oocyte Freezing treatment in Vasant Kunj
- Adenomyosis treatment in Vasant Kunj
- Best ivf centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- Best Infertility treatment in Vasant Vihar
- Best IUI Centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- best ICSI centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Best IVF Doctor in Vasant Vihar
- Low cost IVF Centre in Vasant Vihar
- ovulation Induction Treatment in Vasant Vihar
- Best Embryo transfer Centre in Vasant Vihar
- Best Blastocyst Transfer Centre in Vasant Vihar
- Best Female infertility treatment in Vasant Vihar
- Best Male infertility treatment in Vasant Vihar
- Blocked Fallopian Tubes treatment in Vasant Vihar
- Best PCOS treatment in Vasant Vihar
- Best PCOD treatment in Vasant Vihar
- Polycystic ovaries treatment in Vasant Vihar
- Best Endometriosis Treatment in Vasant Vihar
- unexplained Infertility treatment in Vasant Vihar
- Low AMH in Vasant Vihar
- Poor ovarian reserve treatment in Vasant Vihar
- Poor responder treatment in Vasant Vihar
- Fibroid Uterus treatment in Vasant Vihar
- Myoma in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Hysteroscopy Polypectomy Treatment in Vasant Vihar
- Hysteroscopy septum resection Treatment in Vasant Vihar
- Recurrent Implantation Failure treatment in Vasant Vihar
- Repeated IVF Failure treatment in Vasant Vihar
- PGD Treatment in Vasant Vihar
- PGS Treatment in Vasant Vihar
- Best Oncofertility treatment in Vasant Vihar
- Oocyte Freezing treatment in Vasant Vihar
- Adenomyosis treatment in Vasant Vihar
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best infertility Doctor in Greater Kailash
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best infertility Doctor in Nehru Place
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best infertility Doctor in CR Park
- Best ivf centre in Govindpuri
- Best IVF Centre in Govindpuri
- Best Infertility treatment in Govindpuri
- Best IUI Centre in Govindpuri
- best ICSI centre in Govindpuri
- Best Fertility Doctor in Govindpuri
- Best IVF Doctor in Govindpuri
- Low cost IVF Centre in Govindpuri
- ovulation Induction Treatment in Govindpuri
- Best Embryo transfer Centre in Govindpuri
- Best Blastocyst Transfer Centre in Govindpuri
- Best Female infertility treatment in Govindpuri
- Best Male infertility treatment in Govindpuri
- Blocked Fallopian Tubes treatment in Govindpuri
- Best PCOS treatment in Govindpuri
- Best PCOD treatment in Govindpuri
- Polycystic ovaries treatment in Govindpuri
- Best Endometriosis Treatment in Govindpuri
- unexplained Infertility treatment in Govindpuri
- Low AMH in Govindpuri
- Poor ovarian reserve treatment in Govindpuri
- Poor responder treatment in Govindpuri
- Fibroid Uterus treatment in Govindpuri
- Myoma in Govindpuri
- Endometrial Polyp Treatment in Govindpuri
- Hysteroscopy Polypectomy Treatment in Govindpuri
- Hysteroscopy septum resection Treatment in Govindpuri
- Recurrent Implantation Failure treatment in Govindpuri
- Repeated IVF Failure treatment in Govindpuri
- PGD Treatment in Govindpuri
- PGS Treatment in Govindpuri
- Best Oncofertility treatment in Govindpuri
- Oocyte Freezing treatment in Govindpuri
- Adenomyosis treatment in Govindpuri
- Best infertility Doctor in Govindpuri
- Best IVF Doctor in Saket
- IVF + ICSI Specialist in Saket
- Low Cost IVF Centre in Saket
- Best Fertility Doctor in Saket
- Embryo Transfer Treatment in Saket
- Blastocyst Transfer Treatment in Saket
- Recurrent IVF Failure Treatment in Saket
- Recurrent Implantation Failure Treatment in Saket
- PGD / PGT Treatment in Saket
- PCOS / PCOD Treatment in Saket
- Ovulation Induction Treatment in Saket
- Clomiphene Citrate Treatment in Saket
- Letrozole Treatment in Saket
- Low AMH Treatment in Saket
- Poor ovarian reserve Treatment in Saket
- Laparoscopy Doctor in Saket
- Endometriosis Treatment in Saket
- Fibroid uterus Treatment in Saket
- Hysteroscopy Surgery in Saket
- Hysteroscopy Polypectomy Surgery in Saket
- Endometrial Polyp Treatment in Saket
- Uterine Septum Treatment in Saket
- Adhesiolysis Treatment in Saket
- Female Infertility Treatment in Saket
- Thin Endometrium Treatment in Saket
- Egg Freezing Treatment in Saket
- Oncofertility Treatment in Saket
- Low Sperm count Treatment in Saket
- Azoospermia Treatment in Saket
- Male Infertility Treatment in Saket
- Infertility Treatment in Saket
- Best IVF Doctor in Kalkaji
- IVF + ICSI Specialist in Kalkaji
- Low Cost IVF Centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Embryo Transfer Treatment in Kalkaji
- Blastocyst Transfer Treatment in Kalkaji
- Recurrent IVF Failure Treatment in Kalkaji
- Recurrent Implantation Failure Treatment in Kalkaji
- PGD / PGT Treatment in Kalkaji
- PCOS / PCOD Treatment in Kalkaji
- Ovulation Induction Treatment in Kalkaji
- Clomiphene Citrate Treatment in Kalkaji
- Letrozole Treatment in Kalkaji
- Low AMH Treatment in Kalkaji
- Poor ovarian reserve Treatment in Kalkaji
- Laparoscopy Doctor in Kalkaji
- Endometriosis Treatment in Kalkaji
- Fibroid uterus Treatment in Kalkaji
- Hysteroscopy Surgery in Kalkaji
- Hysteroscopy Polypectomy Surgery in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Uterine Septum Treatment in Kalkaji
- Adhesiolysis Treatment in Kalkaji
- Female Infertility Treatment in Kalkaji
- Thin Endometrium Treatment in Kalkaji
- Egg Freezing Treatment in Kalkaji
- Oncofertility Treatment in Kalkaji
- Low Sperm count Treatment in Kalkaji
- Azoospermia Treatment in Kalkaji
- Male Infertility Treatment in Kalkaji
- Infertility Treatment in Kalkaji
- Best IVF Doctor in CR Park
- IVF + ICSI Specialist in CR Park
- Low Cost IVF Centre in CR Park
- Embryo Transfer Treatment in CR Park
- Blastocyst Transfer Treatment in CR Park
- Recurrent IVF Failure Treatment in CR Park
- Recurrent Implantation Failure Treatment in CR Park
- PGD / PGT Treatment in CR Park
- PCOS / PCOD Treatment in CR Park
- Ovulation Induction Treatment in CR Park
- Clomiphene Citrate Treatment in CR Park
- Letrozole Treatment in CR Park
- Low AMH Treatment in CR Park
- Poor ovarian reserve Treatment in CR Park
- Laparoscopy Doctor in CR Park
- Endometriosis Treatment in CR Park
- Fibroid uterus Treatment in CR Park
- Hysteroscopy Surgery in CR Park
- Hysteroscopy Polypectomy Surgery in CR Park
- Uterine Septum Treatment in CR Park
- Adhesiolysis Treatment in CR Park
- Female Infertility Treatment in CR Park
- Thin Endometrium Treatment in CR Park
- Egg Freezing Treatment in CR Park
- Oncofertility Treatment in CR Park
- Low Sperm count Treatment in CR Park
- Azoospermia Treatment in CR Park
- Male Infertility Treatment in CR Park
- Infertility Treatment in CR Park
- Best IVF Doctor in Nehru Place
- IVF + ICSI Specialist in Nehru Place
- Low Cost IVF Centre in Nehru Place
- Embryo Transfer Treatment in Nehru Place
- Blastocyst Transfer Treatment in Nehru Place
- Recurrent IVF Failure Treatment in Nehru Place
- Recurrent Implantation Failure Treatment in Nehru Place
- PGD / PGT Treatment in Nehru Place
- PCOS / PCOD Treatment in Nehru Place
- Ovulation Induction Treatment in Nehru Place
- Clomiphene Citrate Treatment in Nehru Place
- Letrozole Treatment in Nehru Place
- Low AMH Treatment in Nehru Place
- Poor ovarian reserve Treatment in Nehru Place
- Laparoscopy Doctor in Nehru Place
- Endometriosis Treatment in Nehru Place
- Fibroid uterus Treatment in Nehru Place
- Hysteroscopy Surgery in Nehru Place
- Hysteroscopy Polypectomy Surgery in Nehru Place
- Uterine Septum Treatment in Nehru Place
- Adhesiolysis Treatment in Nehru Place
- Female Infertility Treatment in Nehru Place
- Thin Endometrium Treatment in Nehru Place
- Egg Freezing Treatment in Nehru Place
- Oncofertility Treatment in Nehru Place
- Low Sperm count Treatment in Nehru Place
- Azoospermia Treatment in Nehru Place
- Male Infertility Treatment in Nehru Place
- Infertility Treatment in Nehru Place
- Best IVF Doctor in Greater Kailash
- IVF + ICSI Specialist in Greater Kailash
- Low Cost IVF Centre in Greater Kailash
- Embryo Transfer Treatment in Greater Kailash
- Blastocyst Transfer Treatment in Greater Kailash
- Recurrent IVF Failure Treatment in Greater Kailash
- Recurrent Implantation Failure Treatment in Greater Kailash
- PGD / PGT Treatment in Greater Kailash
- PCOS / PCOD Treatment in Greater Kailash
- Ovulation Induction Treatment in Greater Kailash
- Clomiphene Citrate Treatment in Greater Kailash
- Letrozole Treatment in Greater Kailash
- Low AMH Treatment in Greater Kailash
- Poor ovarian reserve Treatment in Greater Kailash
- Laparoscopy Doctor in Greater Kailash
- Endometriosis Treatment in Greater Kailash
- Fibroid uterus Treatment in Greater Kailash
- Hysteroscopy Surgery in Greater Kailash
- Hysteroscopy Polypectomy Surgery in Greater Kailash
- Uterine Septum Treatment in Greater Kailash
- Adhesiolysis Treatment in Greater Kailash
- Female Infertility Treatment in Greater Kailash
- Thin Endometrium Treatment in Greater Kailash
- Egg Freezing Treatment in Greater Kailash
- Oncofertility Treatment in Greater Kailash
- Low Sperm count Treatment in Greater Kailash
- Azoospermia Treatment in Greater Kailash
- Male Infertility Treatment in Greater Kailash
- Infertility Treatment in Greater Kailash
- '
- Best IVF Doctor in South Delhi
- IVF + ICSI Specialist in South Delhi
- Low Cost IVF Centre in South Delhi
- Best Fertility Doctor in South Delhi
- Embryo Transfer Treatment in South Delhi
- Blastocyst Transfer Treatment in South Delhi
- Recurrent IVF Failure Treatment in South Delhi
- Recurrent Implantation Failure Treatment in South Delhi
- PGD / PGT Treatment in South Delhi
- PCOS / PCOD Treatment in South Delhi
- Ovulation Induction Treatment in South Delhi
- Clomiphene Citrate Treatment in South Delhi
- Letrozole Treatment in South Delhi
- Low AMH Treatment in South Delhi
- Poor ovarian reserve Treatment in South Delhi
- Laparoscopy Doctor in South Delhi
- Endometriosis Treatment in South Delhi
- Fibroid uterus Treatment in South Delhi
- Hysteroscopy Surgery in South Delhi
- Hysteroscopy Polypectomy Surgery in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Uterine Septum Treatment in South Delhi
- Adhesiolysis Treatment in South Delhi
- Female Infertility Treatment in South Delhi
- Thin Endometrium Treatment in South Delhi
- Egg Freezing Treatment in South Delhi
- Oncofertility Treatment in South Delhi
- Low Sperm count Treatment in South Delhi
- Azoospermia Treatment in South Delhi
- Male Infertility Treatment in South Delhi
- Infertility Treatment in South Delhi
- Best IVF Doctor in Malviya Nagar
- IVF + ICSI Specialist in Malviya Nagar
- Low Cost IVF Centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Embryo Transfer Treatment in Malviya Nagar
- Blastocyst Transfer Treatment in Malviya Nagar
- Recurrent IVF Failure Treatment in Malviya Nagar
- Recurrent Implantation Failure Treatment in Malviya Nagar
- PGD / PGT Treatment in Malviya Nagar
- PCOS / PCOD Treatment in Malviya Nagar
- Ovulation Induction Treatment in Malviya Nagar
- Clomiphene Citrate Treatment in Malviya Nagar
- Letrozole Treatment in Malviya Nagar
- Low AMH Treatment in Malviya Nagar
- Poor ovarian reserve Treatment in Malviya Nagar
- Laparoscopy Doctor in Malviya Nagar
- Endometriosis Treatment in Malviya Nagar
- Fibroid uterus Treatment in Malviya Nagar
- Hysteroscopy Surgery in Malviya Nagar
- Hysteroscopy Polypectomy Surgery in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Uterine Septum Treatment in Malviya Nagar
- Adhesiolysis Treatment in Malviya Nagar
- Female Infertility Treatment in Malviya Nagar
- Thin Endometrium Treatment in Malviya Nagar
- Egg Freezing Treatment in Malviya Nagar
- Oncofertility Treatment in Malviya Nagar
- Low Sperm count Treatment in Malviya Nagar
- Azoospermia Treatment in Malviya Nagar
- Male Infertility Treatment in Malviya Nagar
- Infertility Treatment in Malviya Nagar
- Best IVF Doctor in Vasant Kunj
- IVF + ICSI Specialist in Vasant Kunj
- Low Cost IVF Centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Embryo Transfer Treatment in Vasant Kunj
- Blastocyst Transfer Treatment in Vasant Kunj
- Recurrent IVF Failure Treatment in Vasant Kunj
- Recurrent Implantation Failure Treatment in Vasant Kunj
- PGD / PGT Treatment in Vasant Kunj
- PCOS / PCOD Treatment in Vasant Kunj
- Ovulation Induction Treatment in Vasant Kunj
- Clomiphene Citrate Treatment in Vasant Kunj
- Letrozole Treatment in Vasant Kunj
- Low AMH Treatment in Vasant Kunj
- Poor ovarian reserve Treatment in Vasant Kunj
- Laparoscopy Doctor in Vasant Kunj
- Endometriosis Treatment in Vasant Kunj
- Fibroid uterus Treatment in Vasant Kunj
- Hysteroscopy Surgery in Vasant Kunj
- Hysteroscopy Polypectomy Surgery in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Uterine Septum Treatment in Vasant Kunj
- Adhesiolysis Treatment in Vasant Kunj
- Female Infertility Treatment in Vasant Kunj
- Thin Endometrium Treatment in Vasant Kunj
- Egg Freezing Treatment in Vasant Kunj
- Oncofertility Treatment in Vasant Kunj
- Low Sperm count Treatment in Vasant Kunj
- Azoospermia Treatment in Vasant Kunj
- Male Infertility Treatment in Vasant Kunj
- Infertility Treatment in Vasant Kunj
- Best IVF Doctor in Vasant Vihar
- IVF + ICSI Specialist in Vasant Vihar
- Low Cost IVF Centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Embryo Transfer Treatment in Vasant Vihar
- Blastocyst Transfer Treatment in Vasant Vihar
- Recurrent IVF Failure Treatment in Vasant Vihar
- Recurrent Implantation Failure Treatment in Vasant Vihar
- PGD / PGT Treatment in Vasant Vihar
- PCOS / PCOD Treatment in Vasant Vihar
- Ovulation Induction Treatment in Vasant Vihar
- Clomiphene Citrate Treatment in Vasant Vihar
- Letrozole Treatment in Vasant Vihar
- Low AMH Treatment in Vasant Vihar
- Poor ovarian reserve Treatment in Vasant Vihar
- Laparoscopy Doctor in Vasant Vihar
- Endometriosis Treatment in Vasant Vihar
- Fibroid uterus Treatment in Vasant Vihar
- Hysteroscopy Surgery in Vasant Vihar
- Hysteroscopy Polypectomy Surgery in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Uterine Septum Treatment in Vasant Vihar
- Adhesiolysis Treatment in Vasant Vihar
- Female Infertility Treatment in Vasant Vihar
- Thin Endometrium Treatment in Vasant Vihar
- Egg Freezing Treatment in Vasant Vihar
- Oncofertility Treatment in Vasant Vihar
- Low Sperm count Treatment in Vasant Vihar
- Azoospermia Treatment in Vasant Vihar
- Male Infertility Treatment in Vasant Vihar
- Infertility Treatment in Vasant Vihar
- Best IVF Doctor in Govindpuri
- IVF + ICSI Specialist in Govindpuri
- Low Cost IVF Centre in Govindpuri
- Embryo Transfer Treatment in Govindpuri
- Blastocyst Transfer Treatment in Govindpuri
- Recurrent IVF Failure Treatment in Govindpuri
- Recurrent Implantation Failure Treatment in Govindpuri
- PGD / PGT Treatment in Govindpuri
- PCOS / PCOD Treatment in Govindpuri
- Ovulation Induction Treatment in Govindpuri
- Clomiphene Citrate Treatment in Govindpuri
- Letrozole Treatment in Govindpuri
- Low AMH Treatment in Govindpuri
- Poor ovarian reserve Treatment in Govindpuri
- Laparoscopy Doctor in Govindpuri
- Endometriosis Treatment in Govindpuri
- Fibroid uterus Treatment in Govindpuri
- Hysteroscopy Surgery in Govindpuri
- Hysteroscopy Polypectomy Surgery in Govindpuri
- Uterine Septum Treatment in Govindpuri
- Adhesiolysis Treatment in Govindpuri
- Female Infertility Treatment in Govindpuri
- Thin Endometrium Treatment in Govindpuri
- Egg Freezing Treatment in Govindpuri
- Oncofertility Treatment in Govindpuri
- Low Sperm count Treatment in Govindpuri
- Azoospermia Treatment in Govindpuri
- Male Infertility Treatment in Govindpuri
- Infertility Treatment in Govindpuri
- Best IVF centre in Noida
- Best IVF Centre in Noida
- Best Infertility treatment in Noida
- Best IUI Centre in Noida
- Best IVF Centre in Noida
- best ICSI centre in Noida
- Best Fertility Doctor in Noida
- Best IVF Doctor in Noida
- Low-cost IVF Centre in Noida
- ovulation Induction Treatment in Noida
- Best Embryo Transfer Centre in Noida
- Best Blastocyst Transfer Centre in Noida
- Best Female infertility treatment in Noida
- Best Male infertility treatment in Noida
- Blocked Fallopian Tubes treatment in Noida
- Best PCOS treatment in Noida
- Best PCOD treatment in Noida
- Polycystic ovaries treatment in Noida
- Best Endometriosis Treatment in Noida
- unexplained Infertility treatment in Noida
- Low AMH in Noida
- Poor ovarian reserve treatment in Noida
- Poor responder treatment in Noida
- Fibroid Uterus treatment in Noida
- Myoma in Noida
- Endometrial Polyp Treatment in Noida
- Hysteroscopy Polypectomy Treatment in Noida
- Hysteroscopy septum resection Treatment in Noida
- Recurrent Implantation Failure treatment in Noida
- Repeated IVF Failure treatment in Noida
- PGD Treatment in Noida
- PGS Treatment in Noida
- Best Oncofertility treatment in Noida
- Oocyte Freezing treatment in Noida
- Adenomyosis treatment in Noida
- Best Infertility Doctor in Noida
- Best IVF results in Noida
- Best IVF success rate in Noida
- Best IUI results in Noida
- Best IUI success rate in Noida
- Best ICSI centre Low-cost IUI in Noida
- clomiphene citrate in Noida
- Letrozole in Noida
- Donor egg cycle in Noida
- Donor IVF in Noida
- Low sperm count in Noida
- Azoospermia in Noida
- Best infertility Doctor in Delhi
- Best IVF results in Delhi
- Best IVF success rate in Delhi
- Best IUI results in Delhi
- Best IUI success rate in Delhi
- Best ICSI centre in Delhi
- Low cost IUI in Delhi
- clomiphene citrate in Delhi
- Letrozole in Delhi
- Donor egg cycle in Delhi
- Donor IVF in Delhi
- Low sperm count in Delhi
- Azoospermia in Delhi
- Treatment of Azoospermia in Delhi
- Testicular sperm extraction in Delhi
- micro testicular sperm extraction in Delhi
- TESA in Delhi
- TESE in Delhi
- PESA in Delhi
- Microtese in Delhi
- surgical sperm retrieval in Delhi
- Donor sperm IUI in Delhi
- Fibroid uterus in Delhi
- Myomectomy in Delhi
- Laparoscopy in Delhi
- Laparoscopy for Fallopian tube testing in Delhi
- Advanced Laparoscopy in infertility in Delhi
- Diagnostic Laparoscopy in infertility in Delhi
- Hydrosalpinx treatment in Delhi
- Laparoscopy for Hydrosalpinx in Delhi
- Hydrosalpinx in infertility in Delhi
- Laparoscopy for unexplained infertility in Delhi
- Laparoscopy for endometriosis in Delhi
- Endometriotic cyst removal in Delhi
- ovarian cyst in Delhi
- Laparoscopic cyst removal in Delhi
- Hydrosalpinx tubal clipping in Delhi
- Hydrosalpinx salpingectomy in Delhi
- ovarian drilling in Delhi
- laparoscopic ovarian drilling in Delhi
- Hysteroscopy in infertility in Delhi
- pre- IVF Hysteroscopy in Delhi
- Diagnostic Hysteroscopy in Delhi
- Operative Hysteroscopy in Delhi
- Adhesiolysis Hysteroscopy in Delhi
- synechiolysis in Hysteroscopy in Delhi
- synechiae in Delhi
- PGT in Delhi
- Embryo freezing in Delhi
- Frozen Embryo transfer in Delhi
- Fresh embryo transfer in Delhi
- Day 3 embryo transfer in Delhi
- Assissted laser hatching in IVF in Delhi
- Laser hatching in embryo transfer in Delhi
- Blocked Fallopian tubes in Delhi
- egg freezing in Delhi
- embryo freezing in Delhi
- Antagoist protocol in IVF in Delhi
- Long protocol in IVF in Delhi
- Dual stimulation in IVF in Delhi
- Laparoscopy hysterectomy in Delhi
- uterus removal in Delhi
- laparoscopic uterus removal in Delhi
- adenomyomectomy in Delhi
- Adenomyoma in IVF in Delhi
- Mirena insertion in Delhi
- Irregular periods in Delhi
- abnormal uterine bleeding in Delhi
- dysfunctional uterine bleeding in Delhi
- Normal Delivery in Delhi
- Low Cost Delivery in Delhi
- Caesarian in Delhi
- LSCS in Delhi
- Low cost LSCS in Delhi
- Low cost caesarian in Delhi
- Treatment of recurrent abortion in Delhi
- repeated abortion in Delhi
- Thin Endometrium in Delhi
- asherman’s syndrome in Delhi
- ERA in Delhi
- endometrial receptive array in Delhi
- Best infertility Doctor in India
- Best IVF results in India
- Best IVF success rate in India
- Best IUI results in India
- Best IUI success rate in India
- Best ICSI centre in India
- Low cost IUI in India
- clomiphene citrate in India
- Letrozole in India
- Donor egg cycle in India
- Donor IVF in India
- Low sperm count in India
- Azoospermia in India
- Treatment of Azoospermia in India
- Testicular sperm extraction in India
- micro testicular sperm extraction in India
- TESA in India
- TESE in India
- PESA in India
- Microtese in India
- surgical sperm retrieval in India
- Donor sperm IUI in India
- Fibroid uterus in India
- Myomectomy in India
- Laparoscopy in India
- Laparoscopy for Fallopian tube testing in India
- Advanced Laparoscopy in infertility in India
- Diagnostic Laparoscopy in infertility in India
- Hydrosalpinx treatment in India
- Laparoscopy for Hydrosalpinx in India
- Hydrosalpinx in infertility in India
- Laparoscopy for unexplained infertility in India
- Laparoscopy for endometriosis in India
- Endometriotic cyst removal in India
- ovarian cyst in India
- Laparoscopic cyst removal in India
- Hydrosalpinx tubal clipping in India
- Hydrosalpinx salpingectomy in India
- ovarian drilling in India
- laparoscopic ovarian drilling in India
- Hysteroscopy in infertility in India
- pre- IVF Hysteroscopy in India
- Diagnostic Hysteroscopy in India
- Operative Hysteroscopy in India
- Adhesiolysis Hysteroscopy in India
- synechiolysis in Hysteroscopy in India
- synechiae in India
- PGT in India
- Embryo freezing in India
- Frozen Embryo transfer in India
- Fresh embryo transfer in India
- Day 3 embryo transfer in India
- Assissted laser hatching in IVF in India
- Laser hatching in embryo transfer in India
- Blocked Fallopian tubes in India
- egg freezing in India
- embryo freezing in India
- Antagoist protocol in IVF in India
- Long protocol in IVF in India
- Dual stimulation in IVF in India
- Laparoscopy hysterectomy in India
- uterus removal in India
- laparoscopic uterus removal in India
- adenomyomectomy in India
- Adenomyoma in IVF in India
- Mirena insertion in India
- Irregular periods in India
- abnormal uterine bleeding in India
- dysfunctional uterine bleeding in India
- Normal Delivery in India
- Low Cost Delivery in India
- Caesarian in India
- LSCS in India
- Low cost LSCS in India
- Low cost caesarian in India
- Treatment of recurrent abortion in India
- repeated abortion in India
- Thin Endometrium in India
- asherman’s syndrome in India
- ERA in India
- endometrial receptive array in India
- Best ivf centre in Saket
- TESE in saket
- Laparoscopic cyst removal in saket
- ivf centre in South Delhi
- IVF Centre in South Delhi
- Infertility treatment in South Delhi
- IUI Centre in South Delhi
- IVF + ICSI centre in South Delhi
- Low cost IVF in South Delhi
- ovulation Induction in South Delhi
- Embryo transfer in South Delhi
- Blastocyst Transfer in South Delhi
- Female infertility treatment in South Delhi
- Male infertility treatment in South Delhi
- PCOS treatment in South Delhi
- PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Endometriosis in South Delhi
- Endometrial Polyp in South Delhi
- Hysteroscopy Polypectomy in South Delhi
- Hysteroscopy septum resection in Saket
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD in South Delhi
- PGS in South Delhi
- Oncofertility treatment in South Delhi
- Best infertility Doctor in South Delhi
- Best IVF results in South Delhi
- Best IVF success rate in South Delhi
- Best IUI results in South Delhi
- Best IUI success rate in South Delhi
- Best ICSI centre in South Delhi
- Low cost IUI in South Delhi
- clomiphene citrate in South Delhi Letrozole in South Delhi
- Donor egg cycle in South Delhi
- Donor IVF in South Delhi
- Low sperm count in South Delhi
- Azoospermia in South Delhi Treatment of Azoospermia in South Delhi
- Testicular sperm extraction in South Delhi
- micro testicular sperm extraction in South Delhi
- TESA in South Delhi
- TESE in South Delhi
- PESA in South Delhi
- Microtese in South Delhi
- surgical sperm retrieval in South Delhi
- Donor sperm IUI in South Delhi
- Fibroid uterus in South Delhi
- Myomectomy in South Delhi
- Laparoscopy in South Delhi
- Laparoscopy for Fallopian tube testing in South Delhi
- Advanced Laparoscopy in infertility in South Delhi
- Diagnostic Laparoscopy in infertility in South Delhi
- Hydrosalpinx treatment in South Delhi
- Laparoscopy for Hydrosalpinx in South Delhi
- Hydrosalpinx in infertility in South Delhi
- Laparoscopy for unexplained infertility in South Delhi
- Laparoscopy for endometriosis in South Delhi
- Endometriotic cyst removal in South Delhi
- ovarian cyst in South Delhi
- Laparoscopic cyst removal in South Delhi
- Hydrosalpinx tubal clipping in South Delhi
- Hydrosalpinx salpingectomy in South Delhi
- ovarian drilling in South Delhi
- laparoscopic ovarian drilling in South Delhi
- Hysteroscopy in infertility in South Delhi
- pre- IVF Hysteroscopy in South Delhi
- Diagnostic Hysteroscopy in South Delhi
- Operative Hysteroscopy in South Delhi
- Adhesiolysis Hysteroscopy in South Delhi
- synechiolysis in Hysteroscopy in South Delhi
- synechiae in South Delhi
- PGT in South Delhi
- Embryo freezing in South Delhi
- Frozen Embryo transfer in South Delhi
- Fresh embryo transfer in South Delhi
- Day 3 embryo transfer in South Delhi
- Assissted laser hatching in IVF in South Delhi
- Laser hatching in embryo transfer in South Delhi
- Blocked Fallopian tubes in South Delhi
- egg freezing in South Delhi
- embryo freezing in South Delhi
- Antagoist protocol in IVF in South Delhi
- Long protocol in IVF in South Delhi
- Dual stimulation in IVF in South Delhi
- Laparoscopy hysterectomy in South Delhi
- uterus removal in South Delhi
- laparoscopic uterus removal in South Delhi
- adenomyomectomy in South Delhi
- Adenomyoma in IVF in South Delhi
- Mirena insertion in South Delhi
- Irregular periods in South Delhi
- abnormal uterine bleeding in South Delhi
- dysfunctional uterine bleeding in South Delhi
- Normal Delivery in South Delhi
- Low Cost Delivery in South Delhi
- Caesarian in South Delhi
- LSCS in South Delhi
- Low cost LSCS in South Delhi
- Low cost caesarian in South Delhi
- Treatment of recurrent abortion in South Delhi
- repeated abortion in South Delhi
- Thin Endometrium in south Delhi
- asherman’s syndrome in south Delhi
- ERA in south Delhi
- endometrial receptive array in south Delhi
- show more
- show less




