Book an Appointment
PGD PGS PGT

PGD PGS PGT
PGD/PGS is a boon in Assisted Reproductive Techniques /IVF
What is PGD/PGS?
Preimplantation genetic diagnosis (PGD) is a technology widely used in IVF and involves genetic testing of embryos. It allows couples who are at risk of transmitting a genetic disease or chromosomal disorder to have children not affected by that condition.
The desiring couple needs to undergo IVF, the eggs and the sperms are fertilized in the IVF laboratory, the embryos which are created are tested on day3 and more so later on day 5/6 .5-8 cells are removed from the outer layer (Trophoectoderm) of each embryo which will eventually become the placenta, without harming the inner cells (inner cell mass) that will eventually become the baby. The cells removed are sent to the genetic lab for the presence or absence of the relevant mutation or chromosome abnormality. After the biopsy is taken, the embryos are frozen and the embryo transfer is planned next cycle where only healthy and disease-free embryos are transferred. PGD refers to the whole trajectory, from biopsy to embryo selection and transfer.
PGD can be used to identify approximately 2,000 inherited single-gene disorders and is 98 percent accurate in identifying affected and unaffected embryos.
How is PGD different from PGS?
PGD is done for specific genetic disorders like thalassemia and is different from PGS which selects euploid embryos (embryos containing the normal number of chromosomes, which is 46 ) for transfer, in order to increase the efficacy of the IVF cycle.
What is PGT?
The terms PGD and PGS are now being replaced by Preimplantation Genetic Testing (PGT). When done for aneuploidies, it is PGT-A; for monogenic/single gene defects PGT-M; and for chromosomal structural rearrangements, it is PGT-SR. So, what was called PGD is now PGT-M, and what was called PGS is now PGT-A or PGT-SR.
What are the Indications of PGD/PGS?
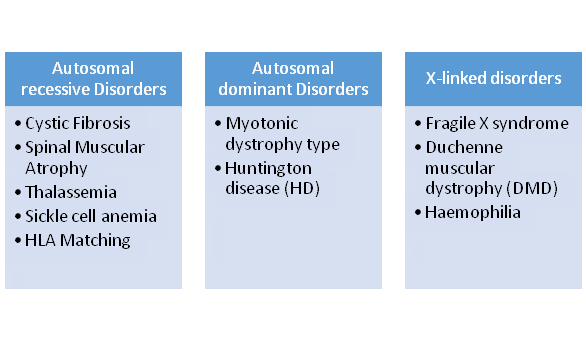
1. The PGD /PGT –M has proved to be very beneficial in single gene disorders which can either be Autosomal recessive, Autosomal Dominant, or X-linked disorders. The various indications are mentioned in the mentioned table.
2. Indications for PGS/ PGT-S/- Structural Chromosomal Abnormalities –. The Chromosomal Structural abnormalities may be the cause of Recurrent Implantation Failure or Recurrent Pregnancy Loss. They are usually Robertsonian, Reciprocal (Male and Female ) sex chromosome abnormalities, etc.
3. Indications for PGS/ PGT-A are – Preimplantation genetic screening is being proposed to improve the effectiveness of in vitro fertilization by screening for embryonic aneuploidy in the following conditions
- Advanced maternal age ( > 35 years)
- Recurrent miscarriage
- Repeated IVF/ICSI –ET failure cycles
- Unexplained infertility
- Severe Male factor
WHAT IS THE ROLE OF PGS IN THE CURRENT SCENARIO?
The application of PGS has become controversial in recent years as eleven randomized control trials (RCTs) (2004-2010) showed that preimplantation genetic screening (PGS) with FISH did not increase delivery rates with some demonstrating adverse outcomes. The possible reason was that only 1-2 cells were biopsied on Day 3 which had a higher rate of mosaicism and were not representative of the rest of the embryo. Moreover FISH detects abnormalities in only 5 chromosomes, embryos diagnosed as euploid by FISH may harbor aneuploidies of other chromosomes that were not tested for. With a shift towards blastocyst biopsy where 5-8 cells can be biopsied instead of 1-2, mosaicism being less and FISH being replaced by newer technologies like array CGH (comparative genomic hybridization ) SNP arrays (single nucleotide polymorphism ), NGS(next generation sequencing ) all chromosomes can be analyzed in a single cell, this approach will result in improved outcomes for PGS.
WHAT ARE THE CONCERNS /DRAWBACKS OF PGD?
The following are considered concerns or disadvantages associated with the use of PGD.
- The process of PGD/PGS requires the couple to undergo IVF even if the couple is fertile which adds to the financial burden on the couple.
- It's an invasive procedure as this requires the manipulation of gametes and embryos involved in IVF/ICSI.
- A condition called mosaicism, where some of the cells in a generally normal embryo are abnormal or some of the cells in a generally abnormal embryo are normal, can lead to test results that do not accurately reflect the chromosome status of the embryo.
- PGD helps in reducing the chances of conceiving a child with a genetic disorder, but it cannot completely eliminate this risk. Further testing is needed such as cell-free fetal DNA testing, chorionic villus sampling (CVS), or amniocentesis during pregnancy to ascertain if a genetic factor is still possible. Therefore, prenatal testing is still recommended and currently remains the standard of care.
- However cumulative data again confirm that pregnancies and babies born after PGD are similar to the pregnancies obtained and babies born after ICSI treatment.
Thus PGD/PGS are highly advanced techniques and especially benefit those couples with genetic disorders by not transferring the mutated genes to their offspring.
PGD /PGS/PGT
Cochrane Data Base Guidelines 2014, for PGD and PGS
Summary:
Preimplantation genetic diagnosis is an alternative to prenatal diagnosis for the detection of genetic disorders in couples at risk of transmitting a genetic condition to their offspring. Preimplantation genetic screening is being proposed to improve the effectiveness of in vitro fertilization by screening for embryonic aneuploidy. Though FISH-based PGS showed adverse effects on IVF success, emerging evidence from new studies using comprehensive chromosome screening technology appears promising.
Recommendations
1. Before a preimplantation genetic diagnosis is performed, genetic counseling must be provided by a certified genetic counselor to ensure that patients fully understand the risk of having an affected child, the impact of the disease on an affected child, and the benefits and limitations of all available options for preimplantation and prenatal diagnosis. (III-A)
2. Couples should be informed that preimplantation genetic diagnosis can reduce the risk of conceiving a child with a genetic abnormality carried by one or both parents if that abnormality can be identified with tests performed on a single cell or on multiple trophectoderm cells. (II-2B) 3. Invasive prenatal or postnatal testing to confirm the results of preimplantation genetic diagnosis is encouraged because the methods used for preimplantation genetic diagnosis have technical limitations that include the possibility of a false result. (II-2B)
4. Trophectoderm biopsy has no measurable impact on embryo development, as opposed to blastomere biopsy. Therefore, whenever possible, trophectoderm biopsy should be the method of choice in embryo biopsy and should be performed by experienced hands. (I-B)
5. Preimplantation genetic diagnosis of single-gene disorders should ideally be performed with multiplex polymerase chain reaction coupled with trophectoderm biopsy whenever available. (II-2B)
6. The use of comprehensive chromosome screening technology coupled with trophectoderm biopsy in preimplantation genetic diagnosis in couples carrying chromosomal translocations is recommended because it is associated with favorable clinical outcomes. (II-2B)
7. Before preimplantation genetic screening is performed, thorough education and counseling must be provided by a certified genetic counselor to ensure that patients fully understand the limitations of the technique, the risk of error, and the ongoing debate on whether preimplantation genetic screening is necessary to improve live birth rates with in vitro fertilization. (III-A)
8. Preimplantation genetic screening using fluorescence in situ hybridization technology on day-3 embryo biopsy is associated with decreased live birth rates and therefore should not be performed with in vitro fertilization. (I-E)
9. Preimplantation genetic screening using comprehensive chromosome screening technology on blastocyst biopsy, increases implantation rates and improves embryo selection in IVF cycles in patients with a good prognosis. (I-B).
Canadian Task Force (CTF), level of evidence
- Level I: Evidence from at least one randomized controlled trial,
- Level II1: Evidence from at least one well-designed cohort study or case-control study, i.e. a controlled trial that is not randomized
- Level II2: Comparisons between times and places with or without the intervention
- Level III: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.
The CTF graded their recommendations on a 5-point A–E scale: A: Good level of evidence for the recommendation to consider a condition, B: Fair level of evidence for the recommendation to consider a condition, C: Poor level of evidence for the recommendation to consider a condition, D: Fair level evidence for the recommendation to exclude the condition, and E: Good level of evidence for the recommendation to exclude the condition from consideration.
Get In Touch
Tags
- Dr. Shalini Gynaecologist
- Dr. Shalini Gynaecologist alaknanda
- Dr. Shalini Chawla Gynaecologist
- Dr. Shalini Chawla Saket
- Best ivf centre in saket
- Best IVF Centre in Saket
- Best Infertility treatment in Saket
- Best IUI Centre in Saket
- Best IVF Centre in Saket
- best ICSI centre in Saket
- Best Fertility Doctor in Saket
- Best IVF Doctor in Saket
- Low cost IVF Centre in Saket
- ovulation Induction Treatment in Saket
- Best Embryo transfer Centre in Saket
- Best Blastocyst Transfer Centre in Saket
- Best Female infertility treatment in Saket
- Best Male infertility treatment in Saket
- Blocked Fallopian Tubes treatment in Saket
- Best PCOS treatment in Saket
- Best PCOD treatment in Saket
- Polycystic ovaries treatment in Saket
- Best Endometriosis Treatment in Saket
- unexplained Infertility treatment in Saket
- Low AMH in Saket
- Poor ovarian reserve treatment in Saket
- Poor responder treatment in Saket
- Fibroid Uterus treatment in Saket
- Myoma in Saket
- Endometrial Polyp Treatment in Saket
- Hysteroscopy Polypectomy Treatment in Saket
- Hysteroscopy septum resection Treatment in Saket
- Recurrent Implantation Failure treatment in Saket
- Repeated IVF Failure treatment in Saket
- PGD Treatment in Saket
- PGS Treatment in Saket
- Best Oncofertility treatment in Saket
- Oocyte Freezing treatment in Saket
- Adenomyosis treatment in Saket
- Best infertility Doctor in Saket
- Best IVF results in saket
- Best IVF success rate in Saket
- Best IUI results in saket
- Best IUI success rate in saket
- Best ICSI centre in saket
- Low cost IUI in saket
- clomiphene citrate in saket
- Letrozole in saket
- Donor egg cycle in saket
- Donor IVF in saket
- Low sperm count in saket
- Azoospermia in saket
- Treatment of Azoospermia in saket
- Testicular sperm extraction in saket
- micro testicular sperm extraction in saket
- TESA in saket
- TESE in saket
- PESA in saket
- Microtese in saket
- surgical sperm retrieval in saket
- Donor sperm IUI in saket
- Fibroid uterus in saket
- Myomectomy in saket
- Laparoscopy in saket
- Laparoscopy for Fallopian tube testing in saket
- Advanced Laparoscopy in infertility in saket
- Diagnostic Laparoscopy in infertility in saket
- Hydrosalpinx treatment in saket
- Laparoscopy for Hydrosalpinx in saket
- Hydrosalpinx in infertility in saket
- Laparoscopy for unexplained infertility in saket
- Laparoscopy for endometriosis in saket
- Endometriotic cyst removal in saket
- ovarian cyst in saket
- Laparoscopic cyst removal in saket
- Hydrosalpinx tubal clipping in saket
- Hydrosalpinx salpingectomy in saket
- ovarian drilling in saket
- laparoscopic ovarian drilling in saket
- Hysteroscopy in infertility in saket
- pre- IVF Hysteroscopy in saket
- Diagnostic Hysteroscopy in saket
- Operative Hysteroscopy in saket
- Adhesiolysis Hysteroscopy in saket
- synechiolysis in Hysteroscopy in saket
- synechiae in saket
- PGT in saket
- Embryo freezing in saket
- Frozen Embryo transfer in saket
- Fresh embryo transfer in saket
- Day 3 embryo transfer in saket
- Assissted laser hatching in IVF in saket
- Laser hatching in embryo transfer in saket
- tuberculosis in infertility in IVF
- Blocked Fallopian tubes in saket
- egg freezing in saket
- embryo freezing in saket
- Antagoist protocol in IVF in saket
- Long protocol in IVF in saket
- Dual stimulation in IVF in saket
- Laparoscopy hysterectomy in saket
- uterus removal in saket
- laparoscopic uterus removal in saket
- adenomyomectomy in saket
- Adenomyoma in IVF in saket
- Mirena insertion in saket
- Irregular periods in saket
- abnormal uterine bleeding in saket
- dysfunctional uterine bleeding in saket
- Normal Delivery in saket
- Low Cost Delivery in saket
- Caesarian in saket
- LSCS in saket
- Low cost LSCS in saket
- Low cost caesarian in saket
- Treatment of recurrent abortion in saket
- repeated abortion in saket
- Thin Endometrium in saket
- asherman’s syndrome in saket
- ERA in saket
- endometrial receptive array in saket
- Best ivf centre in Kalkaji
- Best IVF Centre in Kalkaji
- Best Infertility treatment in Kalkaji
- Best IUI Centre in Kalkaji
- Best IVF Centre in Kalkaji
- best ICSI centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Best IVF Doctor in Kalkaji
- Low cost IVF Centre in Kalkaji
- ovulation Induction Treatment in Kalkaji
- Best Embryo transfer Centre in Kalkaji
- Best Blastocyst Transfer Centre in Kalkaji
- Best Female infertility treatment in Kalkaji
- Best Male infertility treatment in Kalkaji
- Blocked Fallopian Tubes treatment in Kalkaji
- Best PCOS treatment in Kalkaji
- Best PCOD treatment in Kalkaji
- Polycystic ovaries treatment in Kalkaji
- Best Endometriosis Treatment in Kalkaji
- unexplained Infertility treatment in Kalkaji
- Low AMH in Kalkaji
- Poor ovarian reserve treatment in Kalkaji
- Poor responder treatment in Kalkaji
- Fibroid Uterus treatment in Kalkaji
- Myoma in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Hysteroscopy Polypectomy Treatment in Kalkaji
- Hysteroscopy septum resection Treatment in Kalkaji
- Recurrent Implantation Failure treatment in Kalkaji
- Repeated IVF Failure treatment in Kalkaji
- PGD Treatment in Kalkaji
- PGS Treatment in Kalkaji
- Best Oncofertility treatment in Kalkaji
- Oocyte Freezing treatment in Kalkaji
- Adenomyosis treatment in Kalkaji
- Best ivf centre in CR Park
- Best IVF Centre in CR Park
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- Best IVF Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Best Male infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best PCOS treatment in CR Park
- Best PCOD treatment in CR Park
- Polycystic ovaries treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- Recurrent Implantation Failure treatment in CR Park
- Repeated IVF Failure treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best ivf centre in Nehru Place
- Best IVF Centre in Nehru Place
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- Best IVF Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Best Male infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best PCOS treatment in Nehru Place
- Best PCOD treatment in Nehru Place
- Polycystic ovaries treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- Recurrent Implantation Failure treatment in Nehru Place
- Repeated IVF Failure treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best ivf centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Best Male infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best PCOS treatment in Greater Kailash
- Best PCOD treatment in Greater Kailash
- Polycystic ovaries treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- Recurrent Implantation Failure treatment in Greater Kailash
- Repeated IVF Failure treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best ivf centre in South Delhi
- Best IVF Centre in South Delhi
- Best Infertility treatment in South Delhi
- Best IUI Centre in South Delhi
- Best IVF Centre in South Delhi
- best ICSI centre in South Delhi
- Best Fertility Doctor in South Delhi
- Best IVF Doctor in South Delhi
- Low cost IVF Centre in South Delhi
- ovulation Induction Treatment in South Delhi
- Best Embryo transfer Centre in South Delhi
- Best Blastocyst Transfer Centre in South Delhi
- Best Female infertility treatment in South Delhi
- Best Male infertility treatment in South Delhi
- Blocked Fallopian Tubes treatment in South Delhi
- Best PCOS treatment in South Delhi
- Best PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Best Endometriosis Treatment in South Delhi
- unexplained Infertility treatment in South Delhi
- Low AMH in South Delhi
- Poor ovarian reserve treatment in South Delhi
- Poor responder treatment in South Delhi
- Fibroid Uterus treatment in South Delhi
- Myoma in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Hysteroscopy Polypectomy Treatment in South Delhi
- Hysteroscopy septum resection Treatment in South Delhi
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD Treatment in South Delhi
- PGS Treatment in South Delhi
- Best Oncofertility treatment in South Delhi
- Oocyte Freezing treatment in South Delhi
- Adenomyosis treatment in South Delhi
- Best ivf centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- Best Infertility treatment in Malviya Nagar
- Best IUI Centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- best ICSI centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Best IVF Doctor in Malviya Nagar
- Low cost IVF Centre in Malviya Nagar
- ovulation Induction Treatment in Malviya Nagar
- Best Embryo transfer Centre in Malviya Nagar
- Best Blastocyst Transfer Centre in Malviya Nagar
- Best Female infertility treatment in Malviya Nagar
- Best Male infertility treatment in Malviya Nagar
- Blocked Fallopian Tubes treatment in Malviya Nagar
- Best PCOS treatment in Malviya Nagar
- Best PCOD treatment in Malviya Nagar
- Polycystic ovaries treatment in Malviya Nagar
- Best Endometriosis Treatment in Malviya Nagar
- unexplained Infertility treatment in Malviya Nagar
- Low AMH in Malviya Nagar
- Poor ovarian reserve treatment in Malviya Nagar
- Poor responder treatment in Malviya Nagar
- Fibroid Uterus treatment in Malviya Nagar
- Myoma in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Hysteroscopy Polypectomy Treatment in Malviya Nagar
- Hysteroscopy septum resection Treatment in Malviya Nagar
- Recurrent Implantation Failure treatment in Malviya Nagar
- Repeated IVF Failure treatment in Malviya Nagar
- PGD Treatment in Malviya Nagar
- PGS Treatment in Malviya Nagar
- Best Oncofertility treatment in Malviya Nagar
- Oocyte Freezing treatment in Malviya Nagar
- Adenomyosis treatment in Malviya Nagar
- Best ivf centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- Best Infertility treatment in Vasant Kunj
- Best IUI Centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- best ICSI centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Best IVF Doctor in Vasant Kunj
- Low cost IVF Centre in Vasant Kunj
- ovulation Induction Treatment in Vasant Kunj
- Best Embryo transfer Centre in Vasant Kunj
- Best Blastocyst Transfer Centre in Vasant Kunj
- Best Female infertility treatment in Vasant Kunj
- Best Male infertility treatment in Vasant Kunj
- Blocked Fallopian Tubes treatment in Vasant Kunj
- Best PCOS treatment in Vasant Kunj
- Best PCOD treatment in Vasant Kunj
- Polycystic ovaries treatment in Vasant Kunj
- Best Endometriosis Treatment in Vasant Kunj
- unexplained Infertility treatment in Vasant Kunj
- Low AMH in Vasant Kunj
- Poor ovarian reserve treatment in Vasant Kunj
- Poor responder treatment in Vasant Kunj
- Fibroid Uterus treatment in Vasant Kunj
- Myoma in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Hysteroscopy Polypectomy Treatment in Vasant Kunj
- Hysteroscopy septum resection Treatment in Vasant Kunj
- Recurrent Implantation Failure treatment in Vasant Kunj
- Repeated IVF Failure treatment in Vasant Kunj
- PGD Treatment in Vasant Kunj
- PGS Treatment in Vasant Kunj
- Best Oncofertility treatment in Vasant Kunj
- Oocyte Freezing treatment in Vasant Kunj
- Adenomyosis treatment in Vasant Kunj
- Best ivf centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- Best Infertility treatment in Vasant Vihar
- Best IUI Centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- best ICSI centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Best IVF Doctor in Vasant Vihar
- Low cost IVF Centre in Vasant Vihar
- ovulation Induction Treatment in Vasant Vihar
- Best Embryo transfer Centre in Vasant Vihar
- Best Blastocyst Transfer Centre in Vasant Vihar
- Best Female infertility treatment in Vasant Vihar
- Best Male infertility treatment in Vasant Vihar
- Blocked Fallopian Tubes treatment in Vasant Vihar
- Best PCOS treatment in Vasant Vihar
- Best PCOD treatment in Vasant Vihar
- Polycystic ovaries treatment in Vasant Vihar
- Best Endometriosis Treatment in Vasant Vihar
- unexplained Infertility treatment in Vasant Vihar
- Low AMH in Vasant Vihar
- Poor ovarian reserve treatment in Vasant Vihar
- Poor responder treatment in Vasant Vihar
- Fibroid Uterus treatment in Vasant Vihar
- Myoma in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Hysteroscopy Polypectomy Treatment in Vasant Vihar
- Hysteroscopy septum resection Treatment in Vasant Vihar
- Recurrent Implantation Failure treatment in Vasant Vihar
- Repeated IVF Failure treatment in Vasant Vihar
- PGD Treatment in Vasant Vihar
- PGS Treatment in Vasant Vihar
- Best Oncofertility treatment in Vasant Vihar
- Oocyte Freezing treatment in Vasant Vihar
- Adenomyosis treatment in Vasant Vihar
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best infertility Doctor in Greater Kailash
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best infertility Doctor in Nehru Place
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best infertility Doctor in CR Park
- Best ivf centre in Govindpuri
- Best IVF Centre in Govindpuri
- Best Infertility treatment in Govindpuri
- Best IUI Centre in Govindpuri
- best ICSI centre in Govindpuri
- Best Fertility Doctor in Govindpuri
- Best IVF Doctor in Govindpuri
- Low cost IVF Centre in Govindpuri
- ovulation Induction Treatment in Govindpuri
- Best Embryo transfer Centre in Govindpuri
- Best Blastocyst Transfer Centre in Govindpuri
- Best Female infertility treatment in Govindpuri
- Best Male infertility treatment in Govindpuri
- Blocked Fallopian Tubes treatment in Govindpuri
- Best PCOS treatment in Govindpuri
- Best PCOD treatment in Govindpuri
- Polycystic ovaries treatment in Govindpuri
- Best Endometriosis Treatment in Govindpuri
- unexplained Infertility treatment in Govindpuri
- Low AMH in Govindpuri
- Poor ovarian reserve treatment in Govindpuri
- Poor responder treatment in Govindpuri
- Fibroid Uterus treatment in Govindpuri
- Myoma in Govindpuri
- Endometrial Polyp Treatment in Govindpuri
- Hysteroscopy Polypectomy Treatment in Govindpuri
- Hysteroscopy septum resection Treatment in Govindpuri
- Recurrent Implantation Failure treatment in Govindpuri
- Repeated IVF Failure treatment in Govindpuri
- PGD Treatment in Govindpuri
- PGS Treatment in Govindpuri
- Best Oncofertility treatment in Govindpuri
- Oocyte Freezing treatment in Govindpuri
- Adenomyosis treatment in Govindpuri
- Best infertility Doctor in Govindpuri
- Best IVF Doctor in Saket
- IVF + ICSI Specialist in Saket
- Low Cost IVF Centre in Saket
- Best Fertility Doctor in Saket
- Embryo Transfer Treatment in Saket
- Blastocyst Transfer Treatment in Saket
- Recurrent IVF Failure Treatment in Saket
- Recurrent Implantation Failure Treatment in Saket
- PGD / PGT Treatment in Saket
- PCOS / PCOD Treatment in Saket
- Ovulation Induction Treatment in Saket
- Clomiphene Citrate Treatment in Saket
- Letrozole Treatment in Saket
- Low AMH Treatment in Saket
- Poor ovarian reserve Treatment in Saket
- Laparoscopy Doctor in Saket
- Endometriosis Treatment in Saket
- Fibroid uterus Treatment in Saket
- Hysteroscopy Surgery in Saket
- Hysteroscopy Polypectomy Surgery in Saket
- Endometrial Polyp Treatment in Saket
- Uterine Septum Treatment in Saket
- Adhesiolysis Treatment in Saket
- Female Infertility Treatment in Saket
- Thin Endometrium Treatment in Saket
- Egg Freezing Treatment in Saket
- Oncofertility Treatment in Saket
- Low Sperm count Treatment in Saket
- Azoospermia Treatment in Saket
- Male Infertility Treatment in Saket
- Infertility Treatment in Saket
- Best IVF Doctor in Kalkaji
- IVF + ICSI Specialist in Kalkaji
- Low Cost IVF Centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Embryo Transfer Treatment in Kalkaji
- Blastocyst Transfer Treatment in Kalkaji
- Recurrent IVF Failure Treatment in Kalkaji
- Recurrent Implantation Failure Treatment in Kalkaji
- PGD / PGT Treatment in Kalkaji
- PCOS / PCOD Treatment in Kalkaji
- Ovulation Induction Treatment in Kalkaji
- Clomiphene Citrate Treatment in Kalkaji
- Letrozole Treatment in Kalkaji
- Low AMH Treatment in Kalkaji
- Poor ovarian reserve Treatment in Kalkaji
- Laparoscopy Doctor in Kalkaji
- Endometriosis Treatment in Kalkaji
- Fibroid uterus Treatment in Kalkaji
- Hysteroscopy Surgery in Kalkaji
- Hysteroscopy Polypectomy Surgery in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Uterine Septum Treatment in Kalkaji
- Adhesiolysis Treatment in Kalkaji
- Female Infertility Treatment in Kalkaji
- Thin Endometrium Treatment in Kalkaji
- Egg Freezing Treatment in Kalkaji
- Oncofertility Treatment in Kalkaji
- Low Sperm count Treatment in Kalkaji
- Azoospermia Treatment in Kalkaji
- Male Infertility Treatment in Kalkaji
- Infertility Treatment in Kalkaji
- Best IVF Doctor in CR Park
- IVF + ICSI Specialist in CR Park
- Low Cost IVF Centre in CR Park
- Embryo Transfer Treatment in CR Park
- Blastocyst Transfer Treatment in CR Park
- Recurrent IVF Failure Treatment in CR Park
- Recurrent Implantation Failure Treatment in CR Park
- PGD / PGT Treatment in CR Park
- PCOS / PCOD Treatment in CR Park
- Ovulation Induction Treatment in CR Park
- Clomiphene Citrate Treatment in CR Park
- Letrozole Treatment in CR Park
- Low AMH Treatment in CR Park
- Poor ovarian reserve Treatment in CR Park
- Laparoscopy Doctor in CR Park
- Endometriosis Treatment in CR Park
- Fibroid uterus Treatment in CR Park
- Hysteroscopy Surgery in CR Park
- Hysteroscopy Polypectomy Surgery in CR Park
- Uterine Septum Treatment in CR Park
- Adhesiolysis Treatment in CR Park
- Female Infertility Treatment in CR Park
- Thin Endometrium Treatment in CR Park
- Egg Freezing Treatment in CR Park
- Oncofertility Treatment in CR Park
- Low Sperm count Treatment in CR Park
- Azoospermia Treatment in CR Park
- Male Infertility Treatment in CR Park
- Infertility Treatment in CR Park
- Best IVF Doctor in Nehru Place
- IVF + ICSI Specialist in Nehru Place
- Low Cost IVF Centre in Nehru Place
- Embryo Transfer Treatment in Nehru Place
- Blastocyst Transfer Treatment in Nehru Place
- Recurrent IVF Failure Treatment in Nehru Place
- Recurrent Implantation Failure Treatment in Nehru Place
- PGD / PGT Treatment in Nehru Place
- PCOS / PCOD Treatment in Nehru Place
- Ovulation Induction Treatment in Nehru Place
- Clomiphene Citrate Treatment in Nehru Place
- Letrozole Treatment in Nehru Place
- Low AMH Treatment in Nehru Place
- Poor ovarian reserve Treatment in Nehru Place
- Laparoscopy Doctor in Nehru Place
- Endometriosis Treatment in Nehru Place
- Fibroid uterus Treatment in Nehru Place
- Hysteroscopy Surgery in Nehru Place
- Hysteroscopy Polypectomy Surgery in Nehru Place
- Uterine Septum Treatment in Nehru Place
- Adhesiolysis Treatment in Nehru Place
- Female Infertility Treatment in Nehru Place
- Thin Endometrium Treatment in Nehru Place
- Egg Freezing Treatment in Nehru Place
- Oncofertility Treatment in Nehru Place
- Low Sperm count Treatment in Nehru Place
- Azoospermia Treatment in Nehru Place
- Male Infertility Treatment in Nehru Place
- Infertility Treatment in Nehru Place
- Best IVF Doctor in Greater Kailash
- IVF + ICSI Specialist in Greater Kailash
- Low Cost IVF Centre in Greater Kailash
- Embryo Transfer Treatment in Greater Kailash
- Blastocyst Transfer Treatment in Greater Kailash
- Recurrent IVF Failure Treatment in Greater Kailash
- Recurrent Implantation Failure Treatment in Greater Kailash
- PGD / PGT Treatment in Greater Kailash
- PCOS / PCOD Treatment in Greater Kailash
- Ovulation Induction Treatment in Greater Kailash
- Clomiphene Citrate Treatment in Greater Kailash
- Letrozole Treatment in Greater Kailash
- Low AMH Treatment in Greater Kailash
- Poor ovarian reserve Treatment in Greater Kailash
- Laparoscopy Doctor in Greater Kailash
- Endometriosis Treatment in Greater Kailash
- Fibroid uterus Treatment in Greater Kailash
- Hysteroscopy Surgery in Greater Kailash
- Hysteroscopy Polypectomy Surgery in Greater Kailash
- Uterine Septum Treatment in Greater Kailash
- Adhesiolysis Treatment in Greater Kailash
- Female Infertility Treatment in Greater Kailash
- Thin Endometrium Treatment in Greater Kailash
- Egg Freezing Treatment in Greater Kailash
- Oncofertility Treatment in Greater Kailash
- Low Sperm count Treatment in Greater Kailash
- Azoospermia Treatment in Greater Kailash
- Male Infertility Treatment in Greater Kailash
- Infertility Treatment in Greater Kailash
- '
- Best IVF Doctor in South Delhi
- IVF + ICSI Specialist in South Delhi
- Low Cost IVF Centre in South Delhi
- Best Fertility Doctor in South Delhi
- Embryo Transfer Treatment in South Delhi
- Blastocyst Transfer Treatment in South Delhi
- Recurrent IVF Failure Treatment in South Delhi
- Recurrent Implantation Failure Treatment in South Delhi
- PGD / PGT Treatment in South Delhi
- PCOS / PCOD Treatment in South Delhi
- Ovulation Induction Treatment in South Delhi
- Clomiphene Citrate Treatment in South Delhi
- Letrozole Treatment in South Delhi
- Low AMH Treatment in South Delhi
- Poor ovarian reserve Treatment in South Delhi
- Laparoscopy Doctor in South Delhi
- Endometriosis Treatment in South Delhi
- Fibroid uterus Treatment in South Delhi
- Hysteroscopy Surgery in South Delhi
- Hysteroscopy Polypectomy Surgery in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Uterine Septum Treatment in South Delhi
- Adhesiolysis Treatment in South Delhi
- Female Infertility Treatment in South Delhi
- Thin Endometrium Treatment in South Delhi
- Egg Freezing Treatment in South Delhi
- Oncofertility Treatment in South Delhi
- Low Sperm count Treatment in South Delhi
- Azoospermia Treatment in South Delhi
- Male Infertility Treatment in South Delhi
- Infertility Treatment in South Delhi
- Best IVF Doctor in Malviya Nagar
- IVF + ICSI Specialist in Malviya Nagar
- Low Cost IVF Centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Embryo Transfer Treatment in Malviya Nagar
- Blastocyst Transfer Treatment in Malviya Nagar
- Recurrent IVF Failure Treatment in Malviya Nagar
- Recurrent Implantation Failure Treatment in Malviya Nagar
- PGD / PGT Treatment in Malviya Nagar
- PCOS / PCOD Treatment in Malviya Nagar
- Ovulation Induction Treatment in Malviya Nagar
- Clomiphene Citrate Treatment in Malviya Nagar
- Letrozole Treatment in Malviya Nagar
- Low AMH Treatment in Malviya Nagar
- Poor ovarian reserve Treatment in Malviya Nagar
- Laparoscopy Doctor in Malviya Nagar
- Endometriosis Treatment in Malviya Nagar
- Fibroid uterus Treatment in Malviya Nagar
- Hysteroscopy Surgery in Malviya Nagar
- Hysteroscopy Polypectomy Surgery in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Uterine Septum Treatment in Malviya Nagar
- Adhesiolysis Treatment in Malviya Nagar
- Female Infertility Treatment in Malviya Nagar
- Thin Endometrium Treatment in Malviya Nagar
- Egg Freezing Treatment in Malviya Nagar
- Oncofertility Treatment in Malviya Nagar
- Low Sperm count Treatment in Malviya Nagar
- Azoospermia Treatment in Malviya Nagar
- Male Infertility Treatment in Malviya Nagar
- Infertility Treatment in Malviya Nagar
- Best IVF Doctor in Vasant Kunj
- IVF + ICSI Specialist in Vasant Kunj
- Low Cost IVF Centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Embryo Transfer Treatment in Vasant Kunj
- Blastocyst Transfer Treatment in Vasant Kunj
- Recurrent IVF Failure Treatment in Vasant Kunj
- Recurrent Implantation Failure Treatment in Vasant Kunj
- PGD / PGT Treatment in Vasant Kunj
- PCOS / PCOD Treatment in Vasant Kunj
- Ovulation Induction Treatment in Vasant Kunj
- Clomiphene Citrate Treatment in Vasant Kunj
- Letrozole Treatment in Vasant Kunj
- Low AMH Treatment in Vasant Kunj
- Poor ovarian reserve Treatment in Vasant Kunj
- Laparoscopy Doctor in Vasant Kunj
- Endometriosis Treatment in Vasant Kunj
- Fibroid uterus Treatment in Vasant Kunj
- Hysteroscopy Surgery in Vasant Kunj
- Hysteroscopy Polypectomy Surgery in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Uterine Septum Treatment in Vasant Kunj
- Adhesiolysis Treatment in Vasant Kunj
- Female Infertility Treatment in Vasant Kunj
- Thin Endometrium Treatment in Vasant Kunj
- Egg Freezing Treatment in Vasant Kunj
- Oncofertility Treatment in Vasant Kunj
- Low Sperm count Treatment in Vasant Kunj
- Azoospermia Treatment in Vasant Kunj
- Male Infertility Treatment in Vasant Kunj
- Infertility Treatment in Vasant Kunj
- Best IVF Doctor in Vasant Vihar
- IVF + ICSI Specialist in Vasant Vihar
- Low Cost IVF Centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Embryo Transfer Treatment in Vasant Vihar
- Blastocyst Transfer Treatment in Vasant Vihar
- Recurrent IVF Failure Treatment in Vasant Vihar
- Recurrent Implantation Failure Treatment in Vasant Vihar
- PGD / PGT Treatment in Vasant Vihar
- PCOS / PCOD Treatment in Vasant Vihar
- Ovulation Induction Treatment in Vasant Vihar
- Clomiphene Citrate Treatment in Vasant Vihar
- Letrozole Treatment in Vasant Vihar
- Low AMH Treatment in Vasant Vihar
- Poor ovarian reserve Treatment in Vasant Vihar
- Laparoscopy Doctor in Vasant Vihar
- Endometriosis Treatment in Vasant Vihar
- Fibroid uterus Treatment in Vasant Vihar
- Hysteroscopy Surgery in Vasant Vihar
- Hysteroscopy Polypectomy Surgery in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Uterine Septum Treatment in Vasant Vihar
- Adhesiolysis Treatment in Vasant Vihar
- Female Infertility Treatment in Vasant Vihar
- Thin Endometrium Treatment in Vasant Vihar
- Egg Freezing Treatment in Vasant Vihar
- Oncofertility Treatment in Vasant Vihar
- Low Sperm count Treatment in Vasant Vihar
- Azoospermia Treatment in Vasant Vihar
- Male Infertility Treatment in Vasant Vihar
- Infertility Treatment in Vasant Vihar
- Best IVF Doctor in Govindpuri
- IVF + ICSI Specialist in Govindpuri
- Low Cost IVF Centre in Govindpuri
- Embryo Transfer Treatment in Govindpuri
- Blastocyst Transfer Treatment in Govindpuri
- Recurrent IVF Failure Treatment in Govindpuri
- Recurrent Implantation Failure Treatment in Govindpuri
- PGD / PGT Treatment in Govindpuri
- PCOS / PCOD Treatment in Govindpuri
- Ovulation Induction Treatment in Govindpuri
- Clomiphene Citrate Treatment in Govindpuri
- Letrozole Treatment in Govindpuri
- Low AMH Treatment in Govindpuri
- Poor ovarian reserve Treatment in Govindpuri
- Laparoscopy Doctor in Govindpuri
- Endometriosis Treatment in Govindpuri
- Fibroid uterus Treatment in Govindpuri
- Hysteroscopy Surgery in Govindpuri
- Hysteroscopy Polypectomy Surgery in Govindpuri
- Uterine Septum Treatment in Govindpuri
- Adhesiolysis Treatment in Govindpuri
- Female Infertility Treatment in Govindpuri
- Thin Endometrium Treatment in Govindpuri
- Egg Freezing Treatment in Govindpuri
- Oncofertility Treatment in Govindpuri
- Low Sperm count Treatment in Govindpuri
- Azoospermia Treatment in Govindpuri
- Male Infertility Treatment in Govindpuri
- Infertility Treatment in Govindpuri
- Best IVF centre in Noida
- Best IVF Centre in Noida
- Best Infertility treatment in Noida
- Best IUI Centre in Noida
- Best IVF Centre in Noida
- best ICSI centre in Noida
- Best Fertility Doctor in Noida
- Best IVF Doctor in Noida
- Low-cost IVF Centre in Noida
- ovulation Induction Treatment in Noida
- Best Embryo Transfer Centre in Noida
- Best Blastocyst Transfer Centre in Noida
- Best Female infertility treatment in Noida
- Best Male infertility treatment in Noida
- Blocked Fallopian Tubes treatment in Noida
- Best PCOS treatment in Noida
- Best PCOD treatment in Noida
- Polycystic ovaries treatment in Noida
- Best Endometriosis Treatment in Noida
- unexplained Infertility treatment in Noida
- Low AMH in Noida
- Poor ovarian reserve treatment in Noida
- Poor responder treatment in Noida
- Fibroid Uterus treatment in Noida
- Myoma in Noida
- Endometrial Polyp Treatment in Noida
- Hysteroscopy Polypectomy Treatment in Noida
- Hysteroscopy septum resection Treatment in Noida
- Recurrent Implantation Failure treatment in Noida
- Repeated IVF Failure treatment in Noida
- PGD Treatment in Noida
- PGS Treatment in Noida
- Best Oncofertility treatment in Noida
- Oocyte Freezing treatment in Noida
- Adenomyosis treatment in Noida
- Best Infertility Doctor in Noida
- Best IVF results in Noida
- Best IVF success rate in Noida
- Best IUI results in Noida
- Best IUI success rate in Noida
- Best ICSI centre Low-cost IUI in Noida
- clomiphene citrate in Noida
- Letrozole in Noida
- Donor egg cycle in Noida
- Donor IVF in Noida
- Low sperm count in Noida
- Azoospermia in Noida
- Best infertility Doctor in Delhi
- Best IVF results in Delhi
- Best IVF success rate in Delhi
- Best IUI results in Delhi
- Best IUI success rate in Delhi
- Best ICSI centre in Delhi
- Low cost IUI in Delhi
- clomiphene citrate in Delhi
- Letrozole in Delhi
- Donor egg cycle in Delhi
- Donor IVF in Delhi
- Low sperm count in Delhi
- Azoospermia in Delhi
- Treatment of Azoospermia in Delhi
- Testicular sperm extraction in Delhi
- micro testicular sperm extraction in Delhi
- TESA in Delhi
- TESE in Delhi
- PESA in Delhi
- Microtese in Delhi
- surgical sperm retrieval in Delhi
- Donor sperm IUI in Delhi
- Fibroid uterus in Delhi
- Myomectomy in Delhi
- Laparoscopy in Delhi
- Laparoscopy for Fallopian tube testing in Delhi
- Advanced Laparoscopy in infertility in Delhi
- Diagnostic Laparoscopy in infertility in Delhi
- Hydrosalpinx treatment in Delhi
- Laparoscopy for Hydrosalpinx in Delhi
- Hydrosalpinx in infertility in Delhi
- Laparoscopy for unexplained infertility in Delhi
- Laparoscopy for endometriosis in Delhi
- Endometriotic cyst removal in Delhi
- ovarian cyst in Delhi
- Laparoscopic cyst removal in Delhi
- Hydrosalpinx tubal clipping in Delhi
- Hydrosalpinx salpingectomy in Delhi
- ovarian drilling in Delhi
- laparoscopic ovarian drilling in Delhi
- Hysteroscopy in infertility in Delhi
- pre- IVF Hysteroscopy in Delhi
- Diagnostic Hysteroscopy in Delhi
- Operative Hysteroscopy in Delhi
- Adhesiolysis Hysteroscopy in Delhi
- synechiolysis in Hysteroscopy in Delhi
- synechiae in Delhi
- PGT in Delhi
- Embryo freezing in Delhi
- Frozen Embryo transfer in Delhi
- Fresh embryo transfer in Delhi
- Day 3 embryo transfer in Delhi
- Assissted laser hatching in IVF in Delhi
- Laser hatching in embryo transfer in Delhi
- Blocked Fallopian tubes in Delhi
- egg freezing in Delhi
- embryo freezing in Delhi
- Antagoist protocol in IVF in Delhi
- Long protocol in IVF in Delhi
- Dual stimulation in IVF in Delhi
- Laparoscopy hysterectomy in Delhi
- uterus removal in Delhi
- laparoscopic uterus removal in Delhi
- adenomyomectomy in Delhi
- Adenomyoma in IVF in Delhi
- Mirena insertion in Delhi
- Irregular periods in Delhi
- abnormal uterine bleeding in Delhi
- dysfunctional uterine bleeding in Delhi
- Normal Delivery in Delhi
- Low Cost Delivery in Delhi
- Caesarian in Delhi
- LSCS in Delhi
- Low cost LSCS in Delhi
- Low cost caesarian in Delhi
- Treatment of recurrent abortion in Delhi
- repeated abortion in Delhi
- Thin Endometrium in Delhi
- asherman’s syndrome in Delhi
- ERA in Delhi
- endometrial receptive array in Delhi
- Best infertility Doctor in India
- Best IVF results in India
- Best IVF success rate in India
- Best IUI results in India
- Best IUI success rate in India
- Best ICSI centre in India
- Low cost IUI in India
- clomiphene citrate in India
- Letrozole in India
- Donor egg cycle in India
- Donor IVF in India
- Low sperm count in India
- Azoospermia in India
- Treatment of Azoospermia in India
- Testicular sperm extraction in India
- micro testicular sperm extraction in India
- TESA in India
- TESE in India
- PESA in India
- Microtese in India
- surgical sperm retrieval in India
- Donor sperm IUI in India
- Fibroid uterus in India
- Myomectomy in India
- Laparoscopy in India
- Laparoscopy for Fallopian tube testing in India
- Advanced Laparoscopy in infertility in India
- Diagnostic Laparoscopy in infertility in India
- Hydrosalpinx treatment in India
- Laparoscopy for Hydrosalpinx in India
- Hydrosalpinx in infertility in India
- Laparoscopy for unexplained infertility in India
- Laparoscopy for endometriosis in India
- Endometriotic cyst removal in India
- ovarian cyst in India
- Laparoscopic cyst removal in India
- Hydrosalpinx tubal clipping in India
- Hydrosalpinx salpingectomy in India
- ovarian drilling in India
- laparoscopic ovarian drilling in India
- Hysteroscopy in infertility in India
- pre- IVF Hysteroscopy in India
- Diagnostic Hysteroscopy in India
- Operative Hysteroscopy in India
- Adhesiolysis Hysteroscopy in India
- synechiolysis in Hysteroscopy in India
- synechiae in India
- PGT in India
- Embryo freezing in India
- Frozen Embryo transfer in India
- Fresh embryo transfer in India
- Day 3 embryo transfer in India
- Assissted laser hatching in IVF in India
- Laser hatching in embryo transfer in India
- Blocked Fallopian tubes in India
- egg freezing in India
- embryo freezing in India
- Antagoist protocol in IVF in India
- Long protocol in IVF in India
- Dual stimulation in IVF in India
- Laparoscopy hysterectomy in India
- uterus removal in India
- laparoscopic uterus removal in India
- adenomyomectomy in India
- Adenomyoma in IVF in India
- Mirena insertion in India
- Irregular periods in India
- abnormal uterine bleeding in India
- dysfunctional uterine bleeding in India
- Normal Delivery in India
- Low Cost Delivery in India
- Caesarian in India
- LSCS in India
- Low cost LSCS in India
- Low cost caesarian in India
- Treatment of recurrent abortion in India
- repeated abortion in India
- Thin Endometrium in India
- asherman’s syndrome in India
- ERA in India
- endometrial receptive array in India
- Best ivf centre in Saket
- TESE in saket
- Laparoscopic cyst removal in saket
- ivf centre in South Delhi
- IVF Centre in South Delhi
- Infertility treatment in South Delhi
- IUI Centre in South Delhi
- IVF + ICSI centre in South Delhi
- Low cost IVF in South Delhi
- ovulation Induction in South Delhi
- Embryo transfer in South Delhi
- Blastocyst Transfer in South Delhi
- Female infertility treatment in South Delhi
- Male infertility treatment in South Delhi
- PCOS treatment in South Delhi
- PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Endometriosis in South Delhi
- Endometrial Polyp in South Delhi
- Hysteroscopy Polypectomy in South Delhi
- Hysteroscopy septum resection in Saket
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD in South Delhi
- PGS in South Delhi
- Oncofertility treatment in South Delhi
- Best infertility Doctor in South Delhi
- Best IVF results in South Delhi
- Best IVF success rate in South Delhi
- Best IUI results in South Delhi
- Best IUI success rate in South Delhi
- Best ICSI centre in South Delhi
- Low cost IUI in South Delhi
- clomiphene citrate in South Delhi Letrozole in South Delhi
- Donor egg cycle in South Delhi
- Donor IVF in South Delhi
- Low sperm count in South Delhi
- Azoospermia in South Delhi Treatment of Azoospermia in South Delhi
- Testicular sperm extraction in South Delhi
- micro testicular sperm extraction in South Delhi
- TESA in South Delhi
- TESE in South Delhi
- PESA in South Delhi
- Microtese in South Delhi
- surgical sperm retrieval in South Delhi
- Donor sperm IUI in South Delhi
- Fibroid uterus in South Delhi
- Myomectomy in South Delhi
- Laparoscopy in South Delhi
- Laparoscopy for Fallopian tube testing in South Delhi
- Advanced Laparoscopy in infertility in South Delhi
- Diagnostic Laparoscopy in infertility in South Delhi
- Hydrosalpinx treatment in South Delhi
- Laparoscopy for Hydrosalpinx in South Delhi
- Hydrosalpinx in infertility in South Delhi
- Laparoscopy for unexplained infertility in South Delhi
- Laparoscopy for endometriosis in South Delhi
- Endometriotic cyst removal in South Delhi
- ovarian cyst in South Delhi
- Laparoscopic cyst removal in South Delhi
- Hydrosalpinx tubal clipping in South Delhi
- Hydrosalpinx salpingectomy in South Delhi
- ovarian drilling in South Delhi
- laparoscopic ovarian drilling in South Delhi
- Hysteroscopy in infertility in South Delhi
- pre- IVF Hysteroscopy in South Delhi
- Diagnostic Hysteroscopy in South Delhi
- Operative Hysteroscopy in South Delhi
- Adhesiolysis Hysteroscopy in South Delhi
- synechiolysis in Hysteroscopy in South Delhi
- synechiae in South Delhi
- PGT in South Delhi
- Embryo freezing in South Delhi
- Frozen Embryo transfer in South Delhi
- Fresh embryo transfer in South Delhi
- Day 3 embryo transfer in South Delhi
- Assissted laser hatching in IVF in South Delhi
- Laser hatching in embryo transfer in South Delhi
- Blocked Fallopian tubes in South Delhi
- egg freezing in South Delhi
- embryo freezing in South Delhi
- Antagoist protocol in IVF in South Delhi
- Long protocol in IVF in South Delhi
- Dual stimulation in IVF in South Delhi
- Laparoscopy hysterectomy in South Delhi
- uterus removal in South Delhi
- laparoscopic uterus removal in South Delhi
- adenomyomectomy in South Delhi
- Adenomyoma in IVF in South Delhi
- Mirena insertion in South Delhi
- Irregular periods in South Delhi
- abnormal uterine bleeding in South Delhi
- dysfunctional uterine bleeding in South Delhi
- Normal Delivery in South Delhi
- Low Cost Delivery in South Delhi
- Caesarian in South Delhi
- LSCS in South Delhi
- Low cost LSCS in South Delhi
- Low cost caesarian in South Delhi
- Treatment of recurrent abortion in South Delhi
- repeated abortion in South Delhi
- Thin Endometrium in south Delhi
- asherman’s syndrome in south Delhi
- ERA in south Delhi
- endometrial receptive array in south Delhi
- show more
- show less




