Book an Appointment
Thin Endometrium in Infertility

Thin Endometrium in Infertility
Dr. Shalini Chawla Khanna
Senior IVF Consultant
- Mrx X,32 years –P1A1L1
- 1st –NVD -7 years Back
- 2nd-Medical Abortion 5 years back followed by D&C for retained products
- Trying to conceive for 4 years.
- USG shows an 18 mm follicle on Day 13, Endometrial thickness -5 mm, with irregular margins
- History of scanty flow during periods last 3 years.
- HAnalysis –Normal
- SG –B/L Fallopian Tubes Patent
- Semen
Asherman’s syndrome (AS)
- Intrauterine Adhesions(IUA ) -The presence of adhesions inside the uterine cavity and/or endocervix
- Asherman’s Syndrome –IUA +Symptoms (amenorrhea, hypomenorrhea, recurrent pregnancy loss, infertility, and history of abnormal placentation.
- Prevalence of AS in women with impaired fertility -2.8% to 45.5%.
Risk Factors
- >90% of cases with AS occur after pregnancy-related curettage as the basal layer is destroyed.
Incidence of IUA
- After one curettage -10%
- With at least two curettages -30.6%.
How is it Diagnosed?
Diagnosis
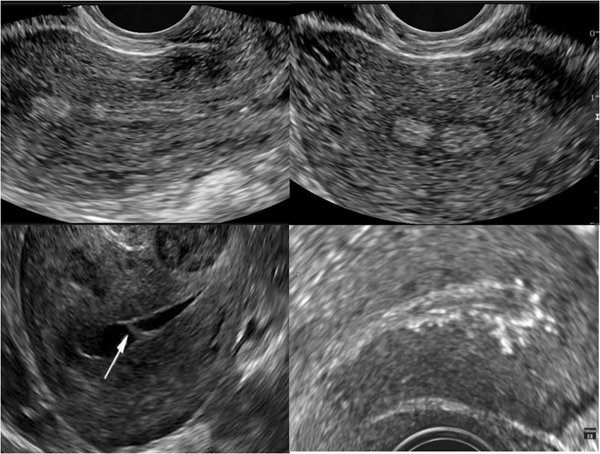
Transvaginal ultrasound-
- Thin Endometrium with irregular Margins
- Echo dense pattern
- Endometrium interrupted by one or more translucent “cyst-like” areas
- Unenhanced transvaginal ultrasonography alone - sensitivity and positive predictive value as low as 0%.
Hysterosalpingography (HSG)
Hysterosalpingography (HSG)-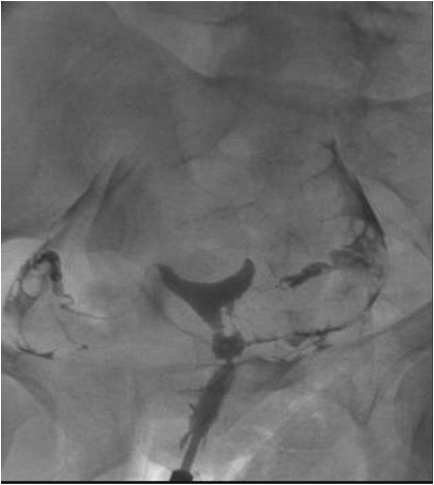
- Filling defects are described as homogeneous opacity surrounded by sharp edges.
- Simultaneous evaluation of Fallopian Tubes.
- High false positive rate
- Saline infusion during the ultrasound scan (sonohysterography or SHG)
- Improves accuracy - 50.3% in the HSG group and 81.8% in the SHG group).
- 3D ultrasound and intrauterine saline infusion (Three-dimensional sonohysterography,3D-SHG)
- Sensitivity and Specificity -91.1% and 98.8%.
MRI
- Especially when totally obliterated uterine cavity
- IUA is visualized as low signal intensity on T2-weighed images inside the uterus [32].
- Expensive
- Hysteroscopy remains the gold standard in the assessment of AS.
Management and treatment of Asherman’s syndrome
The treatment strategy for AS 4 main steps:
- Treatment (Dilatation and curettage, hysteroscopy)
- Re-adhesion prevention (Intrauterine device, Uterine balloon stent, Foley’s catheter, Anti-adhesion Barriers)
- Restoring normal endometrium (Hormonal treatment, stem cells)
- Post-operative assessment (Repeat surgery; diagnostic hysteroscopy; ultrasound).
Hysteroscopic surgery – Principles
- Flimsy Lesions -Tip of the hysteroscope and uterine distension enough to break down the adhesions -” no touch technique’
- Removal of the adhesions should start from the lower part of the uterus and progress toward the upper part.
- Any central and filmy adhesions separated initially in order to allow adequate distension of the uterine cavity.
- Dense and lateral adhesions should be treated at the end - the greater risk of uterine perforation and bleeding.
Hysteroscopic Surgery – Principles
Cold-knife approach> Electric Surgery
- Potential damage to the residual endometrium.
- Bipolar superior to Monopolar -tissue effect is more focal, use of electrolyte-containing uterine distension media - that electrolyte changes are less likely to be clinically serious in cases of fluid overload.
- Laser - Nd-YAG (neodymium-doped yttrium aluminum garnet) and KTP(potassium-titanyl-phosphate)
- Higher costs and increased uterine damages
Prevention of adhesion recurrence
The rate of IUA reformation after surgery remains high (3.1% to 23.5%). These adhesions usually tend to be thin and filmy
IUD
- Helps in Physiological Endometrial Regeneration by separating the anterior and posterior uterine walls.
- Nevertheless, some authors believe that inflammatory factors released by copper devices could aggravate the endometrial injury
- IUD is retained for 2-3 months
- No difference in adhesion reformation among women randomized to receive an IUD device, estrogens treatment, or no treatment after hysteroscopic septum resection Touguc et al.
- The Levonorgestrel-releasing IUD is Not Recommended.
Foley Catheter
- Higher conception rate compared with the IUD group (33.9% versus 22.5%).
- 81% of women restored their normal menstrual pattern.
- Follys catheter- retained inside the uterus for ten days.
- Complication -Uterine perforation, Ascending infection from the vagina, and high discomfort.
Intrauterine balloon stent
- Silicon made -Triangular shape device fits the normal triangular shape of the uterine cavity (Cook Medical Inc, Bloomington, USA).
- 1240 patients treated - Pregnancy rate of 61.6% and spontaneous miscarriage rate of 15.6%.
- No data about IUA recurrence was reported.
- A prophylactic broad-spectrum antibiotic is Recommended to prevent infection.
- Although this is encouraging evidence, data about its safety and efficacy seem still insufficient.
Hyaluronic acid
- Hyaluronic acid generates a temporary barrier between organs which mechanically adhesions formation
- In addition, these products influence peritoneal tissue repair by increasing the proliferation rate of mesothelial cells
- Autocross-linked hyaluronic acid (Hyalobarrier)
- It is a highly viscous gel formed by the autocross-linked condensation of hyaluronic acid
- It can prevent intraperitoneal adhesion after laparoscopic myomectomy and intrauterine adhesions after a hysteroscopic procedure
- Chemically modified hyaluronic acid (sodium hyaluronate) and carboxymethylcellulose (Seprafilm).
- Alginate carboxymethylcellulose hyaluronic acid- Four weeks after surgery, intrauterine adhesions were significantly lower compared with carboxymethylcellulose hyaluronic acid (187 patients )
Restoration of normal endometrium
- Medical therapy –Estrogen
- Encourage fast growth of any residual endometrium immediately after surgery with the dual purpose of preventing new scar formation, increasing endometrial thickness, and restoring a normal uterine environment.
- Estrogen Supplementation -No conclusion on the ideal dosage, the timing of Estorgen, or the route of administration (vaginal or oral).
- 4 mg and 10 mg estradiol orally -No superior effect of the high dosage was demonstrated.
Complications of AS
- Obstetric complications may occur-
- Lower birth weight
- Increased incidence of preterm delivery and retained placenta (placenta accreta in 10.7% of the patients
The success of Hysteroscopy A3
- An overall pregnancy rate from 40% to 63% was previously described.
Stem cells and endometrial regeneration
- Regeneration of endometrium through stem cell treatment has been evaluated both in animal models and in small experimental human studies.
- Bone marrow-derived stem cells, mesenchymal stem cells, and autologous menstrual blood-derived stromal cells have been investigated.
- Different application methods have been used -Infusion in spiral arterioles through catheters, trans myometrial administration to the sub-endometrial area, and direct installation of stromal cells in the uterine cavity after endometrial scratching.
- Future randomized trials are needed to prove if stem cell treatment will have a clinical role in AS
Second-look hysteroscopy
- Post-treatment assessment of the uterine cavity is recommended one-two month after the initial surgery.
- 50% and 21.6% of recurrence in severe and moderate AS respectively
- Second-look hysteroscopy with the division of newly formed adherences ( retrospective study, 151 patients),
- cumulative pregnancy rate (77% vs 56%), and live birth rate (77% vs 63%)
Resistant Thin Endometrium
- Drugs to increase Endometrial Blood Flow –
- Pentoxifylline 800 mg/day
- Tocopherol 1000 mg/day, several months
- Sildenafil 100 mg/day, vaginal pessary
- L‑arginine 6 g/day,
- Low-dose aspirin 75 mg/day.
- None of these therapies have met with much success.
Get In Touch
Tags
- Dr. Shalini Gynaecologist
- Dr. Shalini Gynaecologist alaknanda
- Dr. Shalini Chawla Gynaecologist
- Dr. Shalini Chawla Saket
- Best ivf centre in saket
- Best IVF Centre in Saket
- Best Infertility treatment in Saket
- Best IUI Centre in Saket
- Best IVF Centre in Saket
- best ICSI centre in Saket
- Best Fertility Doctor in Saket
- Best IVF Doctor in Saket
- Low cost IVF Centre in Saket
- ovulation Induction Treatment in Saket
- Best Embryo transfer Centre in Saket
- Best Blastocyst Transfer Centre in Saket
- Best Female infertility treatment in Saket
- Best Male infertility treatment in Saket
- Blocked Fallopian Tubes treatment in Saket
- Best PCOS treatment in Saket
- Best PCOD treatment in Saket
- Polycystic ovaries treatment in Saket
- Best Endometriosis Treatment in Saket
- unexplained Infertility treatment in Saket
- Low AMH in Saket
- Poor ovarian reserve treatment in Saket
- Poor responder treatment in Saket
- Fibroid Uterus treatment in Saket
- Myoma in Saket
- Endometrial Polyp Treatment in Saket
- Hysteroscopy Polypectomy Treatment in Saket
- Hysteroscopy septum resection Treatment in Saket
- Recurrent Implantation Failure treatment in Saket
- Repeated IVF Failure treatment in Saket
- PGD Treatment in Saket
- PGS Treatment in Saket
- Best Oncofertility treatment in Saket
- Oocyte Freezing treatment in Saket
- Adenomyosis treatment in Saket
- Best infertility Doctor in Saket
- Best IVF results in saket
- Best IVF success rate in Saket
- Best IUI results in saket
- Best IUI success rate in saket
- Best ICSI centre in saket
- Low cost IUI in saket
- clomiphene citrate in saket
- Letrozole in saket
- Donor egg cycle in saket
- Donor IVF in saket
- Low sperm count in saket
- Azoospermia in saket
- Treatment of Azoospermia in saket
- Testicular sperm extraction in saket
- micro testicular sperm extraction in saket
- TESA in saket
- TESE in saket
- PESA in saket
- Microtese in saket
- surgical sperm retrieval in saket
- Donor sperm IUI in saket
- Fibroid uterus in saket
- Myomectomy in saket
- Laparoscopy in saket
- Laparoscopy for Fallopian tube testing in saket
- Advanced Laparoscopy in infertility in saket
- Diagnostic Laparoscopy in infertility in saket
- Hydrosalpinx treatment in saket
- Laparoscopy for Hydrosalpinx in saket
- Hydrosalpinx in infertility in saket
- Laparoscopy for unexplained infertility in saket
- Laparoscopy for endometriosis in saket
- Endometriotic cyst removal in saket
- ovarian cyst in saket
- Laparoscopic cyst removal in saket
- Hydrosalpinx tubal clipping in saket
- Hydrosalpinx salpingectomy in saket
- ovarian drilling in saket
- laparoscopic ovarian drilling in saket
- Hysteroscopy in infertility in saket
- pre- IVF Hysteroscopy in saket
- Diagnostic Hysteroscopy in saket
- Operative Hysteroscopy in saket
- Adhesiolysis Hysteroscopy in saket
- synechiolysis in Hysteroscopy in saket
- synechiae in saket
- PGT in saket
- Embryo freezing in saket
- Frozen Embryo transfer in saket
- Fresh embryo transfer in saket
- Day 3 embryo transfer in saket
- Assissted laser hatching in IVF in saket
- Laser hatching in embryo transfer in saket
- tuberculosis in infertility in IVF
- Blocked Fallopian tubes in saket
- egg freezing in saket
- embryo freezing in saket
- Antagoist protocol in IVF in saket
- Long protocol in IVF in saket
- Dual stimulation in IVF in saket
- Laparoscopy hysterectomy in saket
- uterus removal in saket
- laparoscopic uterus removal in saket
- adenomyomectomy in saket
- Adenomyoma in IVF in saket
- Mirena insertion in saket
- Irregular periods in saket
- abnormal uterine bleeding in saket
- dysfunctional uterine bleeding in saket
- Normal Delivery in saket
- Low Cost Delivery in saket
- Caesarian in saket
- LSCS in saket
- Low cost LSCS in saket
- Low cost caesarian in saket
- Treatment of recurrent abortion in saket
- repeated abortion in saket
- Thin Endometrium in saket
- asherman’s syndrome in saket
- ERA in saket
- endometrial receptive array in saket
- Best ivf centre in Kalkaji
- Best IVF Centre in Kalkaji
- Best Infertility treatment in Kalkaji
- Best IUI Centre in Kalkaji
- Best IVF Centre in Kalkaji
- best ICSI centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Best IVF Doctor in Kalkaji
- Low cost IVF Centre in Kalkaji
- ovulation Induction Treatment in Kalkaji
- Best Embryo transfer Centre in Kalkaji
- Best Blastocyst Transfer Centre in Kalkaji
- Best Female infertility treatment in Kalkaji
- Best Male infertility treatment in Kalkaji
- Blocked Fallopian Tubes treatment in Kalkaji
- Best PCOS treatment in Kalkaji
- Best PCOD treatment in Kalkaji
- Polycystic ovaries treatment in Kalkaji
- Best Endometriosis Treatment in Kalkaji
- unexplained Infertility treatment in Kalkaji
- Low AMH in Kalkaji
- Poor ovarian reserve treatment in Kalkaji
- Poor responder treatment in Kalkaji
- Fibroid Uterus treatment in Kalkaji
- Myoma in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Hysteroscopy Polypectomy Treatment in Kalkaji
- Hysteroscopy septum resection Treatment in Kalkaji
- Recurrent Implantation Failure treatment in Kalkaji
- Repeated IVF Failure treatment in Kalkaji
- PGD Treatment in Kalkaji
- PGS Treatment in Kalkaji
- Best Oncofertility treatment in Kalkaji
- Oocyte Freezing treatment in Kalkaji
- Adenomyosis treatment in Kalkaji
- Best ivf centre in CR Park
- Best IVF Centre in CR Park
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- Best IVF Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Best Male infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best PCOS treatment in CR Park
- Best PCOD treatment in CR Park
- Polycystic ovaries treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- Recurrent Implantation Failure treatment in CR Park
- Repeated IVF Failure treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best ivf centre in Nehru Place
- Best IVF Centre in Nehru Place
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- Best IVF Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Best Male infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best PCOS treatment in Nehru Place
- Best PCOD treatment in Nehru Place
- Polycystic ovaries treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- Recurrent Implantation Failure treatment in Nehru Place
- Repeated IVF Failure treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best ivf centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- Best IVF Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Best Male infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best PCOS treatment in Greater Kailash
- Best PCOD treatment in Greater Kailash
- Polycystic ovaries treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- Recurrent Implantation Failure treatment in Greater Kailash
- Repeated IVF Failure treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best ivf centre in South Delhi
- Best IVF Centre in South Delhi
- Best Infertility treatment in South Delhi
- Best IUI Centre in South Delhi
- Best IVF Centre in South Delhi
- best ICSI centre in South Delhi
- Best Fertility Doctor in South Delhi
- Best IVF Doctor in South Delhi
- Low cost IVF Centre in South Delhi
- ovulation Induction Treatment in South Delhi
- Best Embryo transfer Centre in South Delhi
- Best Blastocyst Transfer Centre in South Delhi
- Best Female infertility treatment in South Delhi
- Best Male infertility treatment in South Delhi
- Blocked Fallopian Tubes treatment in South Delhi
- Best PCOS treatment in South Delhi
- Best PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Best Endometriosis Treatment in South Delhi
- unexplained Infertility treatment in South Delhi
- Low AMH in South Delhi
- Poor ovarian reserve treatment in South Delhi
- Poor responder treatment in South Delhi
- Fibroid Uterus treatment in South Delhi
- Myoma in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Hysteroscopy Polypectomy Treatment in South Delhi
- Hysteroscopy septum resection Treatment in South Delhi
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD Treatment in South Delhi
- PGS Treatment in South Delhi
- Best Oncofertility treatment in South Delhi
- Oocyte Freezing treatment in South Delhi
- Adenomyosis treatment in South Delhi
- Best ivf centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- Best Infertility treatment in Malviya Nagar
- Best IUI Centre in Malviya Nagar
- Best IVF Centre in Malviya Nagar
- best ICSI centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Best IVF Doctor in Malviya Nagar
- Low cost IVF Centre in Malviya Nagar
- ovulation Induction Treatment in Malviya Nagar
- Best Embryo transfer Centre in Malviya Nagar
- Best Blastocyst Transfer Centre in Malviya Nagar
- Best Female infertility treatment in Malviya Nagar
- Best Male infertility treatment in Malviya Nagar
- Blocked Fallopian Tubes treatment in Malviya Nagar
- Best PCOS treatment in Malviya Nagar
- Best PCOD treatment in Malviya Nagar
- Polycystic ovaries treatment in Malviya Nagar
- Best Endometriosis Treatment in Malviya Nagar
- unexplained Infertility treatment in Malviya Nagar
- Low AMH in Malviya Nagar
- Poor ovarian reserve treatment in Malviya Nagar
- Poor responder treatment in Malviya Nagar
- Fibroid Uterus treatment in Malviya Nagar
- Myoma in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Hysteroscopy Polypectomy Treatment in Malviya Nagar
- Hysteroscopy septum resection Treatment in Malviya Nagar
- Recurrent Implantation Failure treatment in Malviya Nagar
- Repeated IVF Failure treatment in Malviya Nagar
- PGD Treatment in Malviya Nagar
- PGS Treatment in Malviya Nagar
- Best Oncofertility treatment in Malviya Nagar
- Oocyte Freezing treatment in Malviya Nagar
- Adenomyosis treatment in Malviya Nagar
- Best ivf centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- Best Infertility treatment in Vasant Kunj
- Best IUI Centre in Vasant Kunj
- Best IVF Centre in Vasant Kunj
- best ICSI centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Best IVF Doctor in Vasant Kunj
- Low cost IVF Centre in Vasant Kunj
- ovulation Induction Treatment in Vasant Kunj
- Best Embryo transfer Centre in Vasant Kunj
- Best Blastocyst Transfer Centre in Vasant Kunj
- Best Female infertility treatment in Vasant Kunj
- Best Male infertility treatment in Vasant Kunj
- Blocked Fallopian Tubes treatment in Vasant Kunj
- Best PCOS treatment in Vasant Kunj
- Best PCOD treatment in Vasant Kunj
- Polycystic ovaries treatment in Vasant Kunj
- Best Endometriosis Treatment in Vasant Kunj
- unexplained Infertility treatment in Vasant Kunj
- Low AMH in Vasant Kunj
- Poor ovarian reserve treatment in Vasant Kunj
- Poor responder treatment in Vasant Kunj
- Fibroid Uterus treatment in Vasant Kunj
- Myoma in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Hysteroscopy Polypectomy Treatment in Vasant Kunj
- Hysteroscopy septum resection Treatment in Vasant Kunj
- Recurrent Implantation Failure treatment in Vasant Kunj
- Repeated IVF Failure treatment in Vasant Kunj
- PGD Treatment in Vasant Kunj
- PGS Treatment in Vasant Kunj
- Best Oncofertility treatment in Vasant Kunj
- Oocyte Freezing treatment in Vasant Kunj
- Adenomyosis treatment in Vasant Kunj
- Best ivf centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- Best Infertility treatment in Vasant Vihar
- Best IUI Centre in Vasant Vihar
- Best IVF Centre in Vasant Vihar
- best ICSI centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Best IVF Doctor in Vasant Vihar
- Low cost IVF Centre in Vasant Vihar
- ovulation Induction Treatment in Vasant Vihar
- Best Embryo transfer Centre in Vasant Vihar
- Best Blastocyst Transfer Centre in Vasant Vihar
- Best Female infertility treatment in Vasant Vihar
- Best Male infertility treatment in Vasant Vihar
- Blocked Fallopian Tubes treatment in Vasant Vihar
- Best PCOS treatment in Vasant Vihar
- Best PCOD treatment in Vasant Vihar
- Polycystic ovaries treatment in Vasant Vihar
- Best Endometriosis Treatment in Vasant Vihar
- unexplained Infertility treatment in Vasant Vihar
- Low AMH in Vasant Vihar
- Poor ovarian reserve treatment in Vasant Vihar
- Poor responder treatment in Vasant Vihar
- Fibroid Uterus treatment in Vasant Vihar
- Myoma in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Hysteroscopy Polypectomy Treatment in Vasant Vihar
- Hysteroscopy septum resection Treatment in Vasant Vihar
- Recurrent Implantation Failure treatment in Vasant Vihar
- Repeated IVF Failure treatment in Vasant Vihar
- PGD Treatment in Vasant Vihar
- PGS Treatment in Vasant Vihar
- Best Oncofertility treatment in Vasant Vihar
- Oocyte Freezing treatment in Vasant Vihar
- Adenomyosis treatment in Vasant Vihar
- Best Infertility treatment in Greater Kailash
- Best IUI Centre in Greater Kailash
- best ICSI centre in Greater Kailash
- Best Fertility Doctor in Greater Kailash
- Best IVF Doctor in Greater Kailash
- Low cost IVF Centre in Greater Kailash
- ovulation Induction Treatment in Greater Kailash
- Best Embryo transfer Centre in Greater Kailash
- Best Blastocyst Transfer Centre in Greater Kailash
- Best Female infertility treatment in Greater Kailash
- Blocked Fallopian Tubes treatment in Greater Kailash
- Best Endometriosis Treatment in Greater Kailash
- unexplained Infertility treatment in Greater Kailash
- Low AMH in Greater Kailash
- Poor ovarian reserve treatment in Greater Kailash
- Poor responder treatment in Greater Kailash
- Fibroid Uterus treatment in Greater Kailash
- Myoma in Greater Kailash
- Endometrial Polyp Treatment in Greater Kailash
- Hysteroscopy Polypectomy Treatment in Greater Kailash
- Hysteroscopy septum resection Treatment in Greater Kailash
- PGD Treatment in Greater Kailash
- PGS Treatment in Greater Kailash
- Best Oncofertility treatment in Greater Kailash
- Oocyte Freezing treatment in Greater Kailash
- Adenomyosis treatment in Greater Kailash
- Best infertility Doctor in Greater Kailash
- Best Infertility treatment in Nehru Place
- Best IUI Centre in Nehru Place
- best ICSI centre in Nehru Place
- Best Fertility Doctor in Nehru Place
- Best IVF Doctor in Nehru Place
- Low cost IVF Centre in Nehru Place
- ovulation Induction Treatment in Nehru Place
- Best Embryo transfer Centre in Nehru Place
- Best Blastocyst Transfer Centre in Nehru Place
- Best Female infertility treatment in Nehru Place
- Blocked Fallopian Tubes treatment in Nehru Place
- Best Endometriosis Treatment in Nehru Place
- unexplained Infertility treatment in Nehru Place
- Low AMH in Nehru Place
- Poor ovarian reserve treatment in Nehru Place
- Poor responder treatment in Nehru Place
- Fibroid Uterus treatment in Nehru Place
- Myoma in Nehru Place
- Endometrial Polyp Treatment in Nehru Place
- Hysteroscopy Polypectomy Treatment in Nehru Place
- Hysteroscopy septum resection Treatment in Nehru Place
- PGD Treatment in Nehru Place
- PGS Treatment in Nehru Place
- Best Oncofertility treatment in Nehru Place
- Oocyte Freezing treatment in Nehru Place
- Adenomyosis treatment in Nehru Place
- Best infertility Doctor in Nehru Place
- Best Infertility treatment in CR Park
- Best IUI Centre in CR Park
- best ICSI centre in CR Park
- Best Fertility Doctor in CR Park
- Best IVF Doctor in CR Park
- Low cost IVF Centre in CR Park
- ovulation Induction Treatment in CR Park
- Best Embryo transfer Centre in CR Park
- Best Blastocyst Transfer Centre in CR Park
- Best Female infertility treatment in CR Park
- Blocked Fallopian Tubes treatment in CR Park
- Best Endometriosis Treatment in CR Park
- unexplained Infertility treatment in CR Park
- Low AMH in CR Park
- Poor ovarian reserve treatment in CR Park
- Poor responder treatment in CR Park
- Fibroid Uterus treatment in CR Park
- Myoma in CR Park
- Endometrial Polyp Treatment in CR Park
- Hysteroscopy Polypectomy Treatment in CR Park
- Hysteroscopy septum resection Treatment in CR Park
- PGD Treatment in CR Park
- PGS Treatment in CR Park
- Best Oncofertility treatment in CR Park
- Oocyte Freezing treatment in CR Park
- Adenomyosis treatment in CR Park
- Best infertility Doctor in CR Park
- Best ivf centre in Govindpuri
- Best IVF Centre in Govindpuri
- Best Infertility treatment in Govindpuri
- Best IUI Centre in Govindpuri
- best ICSI centre in Govindpuri
- Best Fertility Doctor in Govindpuri
- Best IVF Doctor in Govindpuri
- Low cost IVF Centre in Govindpuri
- ovulation Induction Treatment in Govindpuri
- Best Embryo transfer Centre in Govindpuri
- Best Blastocyst Transfer Centre in Govindpuri
- Best Female infertility treatment in Govindpuri
- Best Male infertility treatment in Govindpuri
- Blocked Fallopian Tubes treatment in Govindpuri
- Best PCOS treatment in Govindpuri
- Best PCOD treatment in Govindpuri
- Polycystic ovaries treatment in Govindpuri
- Best Endometriosis Treatment in Govindpuri
- unexplained Infertility treatment in Govindpuri
- Low AMH in Govindpuri
- Poor ovarian reserve treatment in Govindpuri
- Poor responder treatment in Govindpuri
- Fibroid Uterus treatment in Govindpuri
- Myoma in Govindpuri
- Endometrial Polyp Treatment in Govindpuri
- Hysteroscopy Polypectomy Treatment in Govindpuri
- Hysteroscopy septum resection Treatment in Govindpuri
- Recurrent Implantation Failure treatment in Govindpuri
- Repeated IVF Failure treatment in Govindpuri
- PGD Treatment in Govindpuri
- PGS Treatment in Govindpuri
- Best Oncofertility treatment in Govindpuri
- Oocyte Freezing treatment in Govindpuri
- Adenomyosis treatment in Govindpuri
- Best infertility Doctor in Govindpuri
- Best IVF Doctor in Saket
- IVF + ICSI Specialist in Saket
- Low Cost IVF Centre in Saket
- Best Fertility Doctor in Saket
- Embryo Transfer Treatment in Saket
- Blastocyst Transfer Treatment in Saket
- Recurrent IVF Failure Treatment in Saket
- Recurrent Implantation Failure Treatment in Saket
- PGD / PGT Treatment in Saket
- PCOS / PCOD Treatment in Saket
- Ovulation Induction Treatment in Saket
- Clomiphene Citrate Treatment in Saket
- Letrozole Treatment in Saket
- Low AMH Treatment in Saket
- Poor ovarian reserve Treatment in Saket
- Laparoscopy Doctor in Saket
- Endometriosis Treatment in Saket
- Fibroid uterus Treatment in Saket
- Hysteroscopy Surgery in Saket
- Hysteroscopy Polypectomy Surgery in Saket
- Endometrial Polyp Treatment in Saket
- Uterine Septum Treatment in Saket
- Adhesiolysis Treatment in Saket
- Female Infertility Treatment in Saket
- Thin Endometrium Treatment in Saket
- Egg Freezing Treatment in Saket
- Oncofertility Treatment in Saket
- Low Sperm count Treatment in Saket
- Azoospermia Treatment in Saket
- Male Infertility Treatment in Saket
- Infertility Treatment in Saket
- Best IVF Doctor in Kalkaji
- IVF + ICSI Specialist in Kalkaji
- Low Cost IVF Centre in Kalkaji
- Best Fertility Doctor in Kalkaji
- Embryo Transfer Treatment in Kalkaji
- Blastocyst Transfer Treatment in Kalkaji
- Recurrent IVF Failure Treatment in Kalkaji
- Recurrent Implantation Failure Treatment in Kalkaji
- PGD / PGT Treatment in Kalkaji
- PCOS / PCOD Treatment in Kalkaji
- Ovulation Induction Treatment in Kalkaji
- Clomiphene Citrate Treatment in Kalkaji
- Letrozole Treatment in Kalkaji
- Low AMH Treatment in Kalkaji
- Poor ovarian reserve Treatment in Kalkaji
- Laparoscopy Doctor in Kalkaji
- Endometriosis Treatment in Kalkaji
- Fibroid uterus Treatment in Kalkaji
- Hysteroscopy Surgery in Kalkaji
- Hysteroscopy Polypectomy Surgery in Kalkaji
- Endometrial Polyp Treatment in Kalkaji
- Uterine Septum Treatment in Kalkaji
- Adhesiolysis Treatment in Kalkaji
- Female Infertility Treatment in Kalkaji
- Thin Endometrium Treatment in Kalkaji
- Egg Freezing Treatment in Kalkaji
- Oncofertility Treatment in Kalkaji
- Low Sperm count Treatment in Kalkaji
- Azoospermia Treatment in Kalkaji
- Male Infertility Treatment in Kalkaji
- Infertility Treatment in Kalkaji
- Best IVF Doctor in CR Park
- IVF + ICSI Specialist in CR Park
- Low Cost IVF Centre in CR Park
- Embryo Transfer Treatment in CR Park
- Blastocyst Transfer Treatment in CR Park
- Recurrent IVF Failure Treatment in CR Park
- Recurrent Implantation Failure Treatment in CR Park
- PGD / PGT Treatment in CR Park
- PCOS / PCOD Treatment in CR Park
- Ovulation Induction Treatment in CR Park
- Clomiphene Citrate Treatment in CR Park
- Letrozole Treatment in CR Park
- Low AMH Treatment in CR Park
- Poor ovarian reserve Treatment in CR Park
- Laparoscopy Doctor in CR Park
- Endometriosis Treatment in CR Park
- Fibroid uterus Treatment in CR Park
- Hysteroscopy Surgery in CR Park
- Hysteroscopy Polypectomy Surgery in CR Park
- Uterine Septum Treatment in CR Park
- Adhesiolysis Treatment in CR Park
- Female Infertility Treatment in CR Park
- Thin Endometrium Treatment in CR Park
- Egg Freezing Treatment in CR Park
- Oncofertility Treatment in CR Park
- Low Sperm count Treatment in CR Park
- Azoospermia Treatment in CR Park
- Male Infertility Treatment in CR Park
- Infertility Treatment in CR Park
- Best IVF Doctor in Nehru Place
- IVF + ICSI Specialist in Nehru Place
- Low Cost IVF Centre in Nehru Place
- Embryo Transfer Treatment in Nehru Place
- Blastocyst Transfer Treatment in Nehru Place
- Recurrent IVF Failure Treatment in Nehru Place
- Recurrent Implantation Failure Treatment in Nehru Place
- PGD / PGT Treatment in Nehru Place
- PCOS / PCOD Treatment in Nehru Place
- Ovulation Induction Treatment in Nehru Place
- Clomiphene Citrate Treatment in Nehru Place
- Letrozole Treatment in Nehru Place
- Low AMH Treatment in Nehru Place
- Poor ovarian reserve Treatment in Nehru Place
- Laparoscopy Doctor in Nehru Place
- Endometriosis Treatment in Nehru Place
- Fibroid uterus Treatment in Nehru Place
- Hysteroscopy Surgery in Nehru Place
- Hysteroscopy Polypectomy Surgery in Nehru Place
- Uterine Septum Treatment in Nehru Place
- Adhesiolysis Treatment in Nehru Place
- Female Infertility Treatment in Nehru Place
- Thin Endometrium Treatment in Nehru Place
- Egg Freezing Treatment in Nehru Place
- Oncofertility Treatment in Nehru Place
- Low Sperm count Treatment in Nehru Place
- Azoospermia Treatment in Nehru Place
- Male Infertility Treatment in Nehru Place
- Infertility Treatment in Nehru Place
- Best IVF Doctor in Greater Kailash
- IVF + ICSI Specialist in Greater Kailash
- Low Cost IVF Centre in Greater Kailash
- Embryo Transfer Treatment in Greater Kailash
- Blastocyst Transfer Treatment in Greater Kailash
- Recurrent IVF Failure Treatment in Greater Kailash
- Recurrent Implantation Failure Treatment in Greater Kailash
- PGD / PGT Treatment in Greater Kailash
- PCOS / PCOD Treatment in Greater Kailash
- Ovulation Induction Treatment in Greater Kailash
- Clomiphene Citrate Treatment in Greater Kailash
- Letrozole Treatment in Greater Kailash
- Low AMH Treatment in Greater Kailash
- Poor ovarian reserve Treatment in Greater Kailash
- Laparoscopy Doctor in Greater Kailash
- Endometriosis Treatment in Greater Kailash
- Fibroid uterus Treatment in Greater Kailash
- Hysteroscopy Surgery in Greater Kailash
- Hysteroscopy Polypectomy Surgery in Greater Kailash
- Uterine Septum Treatment in Greater Kailash
- Adhesiolysis Treatment in Greater Kailash
- Female Infertility Treatment in Greater Kailash
- Thin Endometrium Treatment in Greater Kailash
- Egg Freezing Treatment in Greater Kailash
- Oncofertility Treatment in Greater Kailash
- Low Sperm count Treatment in Greater Kailash
- Azoospermia Treatment in Greater Kailash
- Male Infertility Treatment in Greater Kailash
- Infertility Treatment in Greater Kailash
- '
- Best IVF Doctor in South Delhi
- IVF + ICSI Specialist in South Delhi
- Low Cost IVF Centre in South Delhi
- Best Fertility Doctor in South Delhi
- Embryo Transfer Treatment in South Delhi
- Blastocyst Transfer Treatment in South Delhi
- Recurrent IVF Failure Treatment in South Delhi
- Recurrent Implantation Failure Treatment in South Delhi
- PGD / PGT Treatment in South Delhi
- PCOS / PCOD Treatment in South Delhi
- Ovulation Induction Treatment in South Delhi
- Clomiphene Citrate Treatment in South Delhi
- Letrozole Treatment in South Delhi
- Low AMH Treatment in South Delhi
- Poor ovarian reserve Treatment in South Delhi
- Laparoscopy Doctor in South Delhi
- Endometriosis Treatment in South Delhi
- Fibroid uterus Treatment in South Delhi
- Hysteroscopy Surgery in South Delhi
- Hysteroscopy Polypectomy Surgery in South Delhi
- Endometrial Polyp Treatment in South Delhi
- Uterine Septum Treatment in South Delhi
- Adhesiolysis Treatment in South Delhi
- Female Infertility Treatment in South Delhi
- Thin Endometrium Treatment in South Delhi
- Egg Freezing Treatment in South Delhi
- Oncofertility Treatment in South Delhi
- Low Sperm count Treatment in South Delhi
- Azoospermia Treatment in South Delhi
- Male Infertility Treatment in South Delhi
- Infertility Treatment in South Delhi
- Best IVF Doctor in Malviya Nagar
- IVF + ICSI Specialist in Malviya Nagar
- Low Cost IVF Centre in Malviya Nagar
- Best Fertility Doctor in Malviya Nagar
- Embryo Transfer Treatment in Malviya Nagar
- Blastocyst Transfer Treatment in Malviya Nagar
- Recurrent IVF Failure Treatment in Malviya Nagar
- Recurrent Implantation Failure Treatment in Malviya Nagar
- PGD / PGT Treatment in Malviya Nagar
- PCOS / PCOD Treatment in Malviya Nagar
- Ovulation Induction Treatment in Malviya Nagar
- Clomiphene Citrate Treatment in Malviya Nagar
- Letrozole Treatment in Malviya Nagar
- Low AMH Treatment in Malviya Nagar
- Poor ovarian reserve Treatment in Malviya Nagar
- Laparoscopy Doctor in Malviya Nagar
- Endometriosis Treatment in Malviya Nagar
- Fibroid uterus Treatment in Malviya Nagar
- Hysteroscopy Surgery in Malviya Nagar
- Hysteroscopy Polypectomy Surgery in Malviya Nagar
- Endometrial Polyp Treatment in Malviya Nagar
- Uterine Septum Treatment in Malviya Nagar
- Adhesiolysis Treatment in Malviya Nagar
- Female Infertility Treatment in Malviya Nagar
- Thin Endometrium Treatment in Malviya Nagar
- Egg Freezing Treatment in Malviya Nagar
- Oncofertility Treatment in Malviya Nagar
- Low Sperm count Treatment in Malviya Nagar
- Azoospermia Treatment in Malviya Nagar
- Male Infertility Treatment in Malviya Nagar
- Infertility Treatment in Malviya Nagar
- Best IVF Doctor in Vasant Kunj
- IVF + ICSI Specialist in Vasant Kunj
- Low Cost IVF Centre in Vasant Kunj
- Best Fertility Doctor in Vasant Kunj
- Embryo Transfer Treatment in Vasant Kunj
- Blastocyst Transfer Treatment in Vasant Kunj
- Recurrent IVF Failure Treatment in Vasant Kunj
- Recurrent Implantation Failure Treatment in Vasant Kunj
- PGD / PGT Treatment in Vasant Kunj
- PCOS / PCOD Treatment in Vasant Kunj
- Ovulation Induction Treatment in Vasant Kunj
- Clomiphene Citrate Treatment in Vasant Kunj
- Letrozole Treatment in Vasant Kunj
- Low AMH Treatment in Vasant Kunj
- Poor ovarian reserve Treatment in Vasant Kunj
- Laparoscopy Doctor in Vasant Kunj
- Endometriosis Treatment in Vasant Kunj
- Fibroid uterus Treatment in Vasant Kunj
- Hysteroscopy Surgery in Vasant Kunj
- Hysteroscopy Polypectomy Surgery in Vasant Kunj
- Endometrial Polyp Treatment in Vasant Kunj
- Uterine Septum Treatment in Vasant Kunj
- Adhesiolysis Treatment in Vasant Kunj
- Female Infertility Treatment in Vasant Kunj
- Thin Endometrium Treatment in Vasant Kunj
- Egg Freezing Treatment in Vasant Kunj
- Oncofertility Treatment in Vasant Kunj
- Low Sperm count Treatment in Vasant Kunj
- Azoospermia Treatment in Vasant Kunj
- Male Infertility Treatment in Vasant Kunj
- Infertility Treatment in Vasant Kunj
- Best IVF Doctor in Vasant Vihar
- IVF + ICSI Specialist in Vasant Vihar
- Low Cost IVF Centre in Vasant Vihar
- Best Fertility Doctor in Vasant Vihar
- Embryo Transfer Treatment in Vasant Vihar
- Blastocyst Transfer Treatment in Vasant Vihar
- Recurrent IVF Failure Treatment in Vasant Vihar
- Recurrent Implantation Failure Treatment in Vasant Vihar
- PGD / PGT Treatment in Vasant Vihar
- PCOS / PCOD Treatment in Vasant Vihar
- Ovulation Induction Treatment in Vasant Vihar
- Clomiphene Citrate Treatment in Vasant Vihar
- Letrozole Treatment in Vasant Vihar
- Low AMH Treatment in Vasant Vihar
- Poor ovarian reserve Treatment in Vasant Vihar
- Laparoscopy Doctor in Vasant Vihar
- Endometriosis Treatment in Vasant Vihar
- Fibroid uterus Treatment in Vasant Vihar
- Hysteroscopy Surgery in Vasant Vihar
- Hysteroscopy Polypectomy Surgery in Vasant Vihar
- Endometrial Polyp Treatment in Vasant Vihar
- Uterine Septum Treatment in Vasant Vihar
- Adhesiolysis Treatment in Vasant Vihar
- Female Infertility Treatment in Vasant Vihar
- Thin Endometrium Treatment in Vasant Vihar
- Egg Freezing Treatment in Vasant Vihar
- Oncofertility Treatment in Vasant Vihar
- Low Sperm count Treatment in Vasant Vihar
- Azoospermia Treatment in Vasant Vihar
- Male Infertility Treatment in Vasant Vihar
- Infertility Treatment in Vasant Vihar
- Best IVF Doctor in Govindpuri
- IVF + ICSI Specialist in Govindpuri
- Low Cost IVF Centre in Govindpuri
- Embryo Transfer Treatment in Govindpuri
- Blastocyst Transfer Treatment in Govindpuri
- Recurrent IVF Failure Treatment in Govindpuri
- Recurrent Implantation Failure Treatment in Govindpuri
- PGD / PGT Treatment in Govindpuri
- PCOS / PCOD Treatment in Govindpuri
- Ovulation Induction Treatment in Govindpuri
- Clomiphene Citrate Treatment in Govindpuri
- Letrozole Treatment in Govindpuri
- Low AMH Treatment in Govindpuri
- Poor ovarian reserve Treatment in Govindpuri
- Laparoscopy Doctor in Govindpuri
- Endometriosis Treatment in Govindpuri
- Fibroid uterus Treatment in Govindpuri
- Hysteroscopy Surgery in Govindpuri
- Hysteroscopy Polypectomy Surgery in Govindpuri
- Uterine Septum Treatment in Govindpuri
- Adhesiolysis Treatment in Govindpuri
- Female Infertility Treatment in Govindpuri
- Thin Endometrium Treatment in Govindpuri
- Egg Freezing Treatment in Govindpuri
- Oncofertility Treatment in Govindpuri
- Low Sperm count Treatment in Govindpuri
- Azoospermia Treatment in Govindpuri
- Male Infertility Treatment in Govindpuri
- Infertility Treatment in Govindpuri
- Best IVF centre in Noida
- Best IVF Centre in Noida
- Best Infertility treatment in Noida
- Best IUI Centre in Noida
- Best IVF Centre in Noida
- best ICSI centre in Noida
- Best Fertility Doctor in Noida
- Best IVF Doctor in Noida
- Low-cost IVF Centre in Noida
- ovulation Induction Treatment in Noida
- Best Embryo Transfer Centre in Noida
- Best Blastocyst Transfer Centre in Noida
- Best Female infertility treatment in Noida
- Best Male infertility treatment in Noida
- Blocked Fallopian Tubes treatment in Noida
- Best PCOS treatment in Noida
- Best PCOD treatment in Noida
- Polycystic ovaries treatment in Noida
- Best Endometriosis Treatment in Noida
- unexplained Infertility treatment in Noida
- Low AMH in Noida
- Poor ovarian reserve treatment in Noida
- Poor responder treatment in Noida
- Fibroid Uterus treatment in Noida
- Myoma in Noida
- Endometrial Polyp Treatment in Noida
- Hysteroscopy Polypectomy Treatment in Noida
- Hysteroscopy septum resection Treatment in Noida
- Recurrent Implantation Failure treatment in Noida
- Repeated IVF Failure treatment in Noida
- PGD Treatment in Noida
- PGS Treatment in Noida
- Best Oncofertility treatment in Noida
- Oocyte Freezing treatment in Noida
- Adenomyosis treatment in Noida
- Best Infertility Doctor in Noida
- Best IVF results in Noida
- Best IVF success rate in Noida
- Best IUI results in Noida
- Best IUI success rate in Noida
- Best ICSI centre Low-cost IUI in Noida
- clomiphene citrate in Noida
- Letrozole in Noida
- Donor egg cycle in Noida
- Donor IVF in Noida
- Low sperm count in Noida
- Azoospermia in Noida
- Best infertility Doctor in Delhi
- Best IVF results in Delhi
- Best IVF success rate in Delhi
- Best IUI results in Delhi
- Best IUI success rate in Delhi
- Best ICSI centre in Delhi
- Low cost IUI in Delhi
- clomiphene citrate in Delhi
- Letrozole in Delhi
- Donor egg cycle in Delhi
- Donor IVF in Delhi
- Low sperm count in Delhi
- Azoospermia in Delhi
- Treatment of Azoospermia in Delhi
- Testicular sperm extraction in Delhi
- micro testicular sperm extraction in Delhi
- TESA in Delhi
- TESE in Delhi
- PESA in Delhi
- Microtese in Delhi
- surgical sperm retrieval in Delhi
- Donor sperm IUI in Delhi
- Fibroid uterus in Delhi
- Myomectomy in Delhi
- Laparoscopy in Delhi
- Laparoscopy for Fallopian tube testing in Delhi
- Advanced Laparoscopy in infertility in Delhi
- Diagnostic Laparoscopy in infertility in Delhi
- Hydrosalpinx treatment in Delhi
- Laparoscopy for Hydrosalpinx in Delhi
- Hydrosalpinx in infertility in Delhi
- Laparoscopy for unexplained infertility in Delhi
- Laparoscopy for endometriosis in Delhi
- Endometriotic cyst removal in Delhi
- ovarian cyst in Delhi
- Laparoscopic cyst removal in Delhi
- Hydrosalpinx tubal clipping in Delhi
- Hydrosalpinx salpingectomy in Delhi
- ovarian drilling in Delhi
- laparoscopic ovarian drilling in Delhi
- Hysteroscopy in infertility in Delhi
- pre- IVF Hysteroscopy in Delhi
- Diagnostic Hysteroscopy in Delhi
- Operative Hysteroscopy in Delhi
- Adhesiolysis Hysteroscopy in Delhi
- synechiolysis in Hysteroscopy in Delhi
- synechiae in Delhi
- PGT in Delhi
- Embryo freezing in Delhi
- Frozen Embryo transfer in Delhi
- Fresh embryo transfer in Delhi
- Day 3 embryo transfer in Delhi
- Assissted laser hatching in IVF in Delhi
- Laser hatching in embryo transfer in Delhi
- Blocked Fallopian tubes in Delhi
- egg freezing in Delhi
- embryo freezing in Delhi
- Antagoist protocol in IVF in Delhi
- Long protocol in IVF in Delhi
- Dual stimulation in IVF in Delhi
- Laparoscopy hysterectomy in Delhi
- uterus removal in Delhi
- laparoscopic uterus removal in Delhi
- adenomyomectomy in Delhi
- Adenomyoma in IVF in Delhi
- Mirena insertion in Delhi
- Irregular periods in Delhi
- abnormal uterine bleeding in Delhi
- dysfunctional uterine bleeding in Delhi
- Normal Delivery in Delhi
- Low Cost Delivery in Delhi
- Caesarian in Delhi
- LSCS in Delhi
- Low cost LSCS in Delhi
- Low cost caesarian in Delhi
- Treatment of recurrent abortion in Delhi
- repeated abortion in Delhi
- Thin Endometrium in Delhi
- asherman’s syndrome in Delhi
- ERA in Delhi
- endometrial receptive array in Delhi
- Best infertility Doctor in India
- Best IVF results in India
- Best IVF success rate in India
- Best IUI results in India
- Best IUI success rate in India
- Best ICSI centre in India
- Low cost IUI in India
- clomiphene citrate in India
- Letrozole in India
- Donor egg cycle in India
- Donor IVF in India
- Low sperm count in India
- Azoospermia in India
- Treatment of Azoospermia in India
- Testicular sperm extraction in India
- micro testicular sperm extraction in India
- TESA in India
- TESE in India
- PESA in India
- Microtese in India
- surgical sperm retrieval in India
- Donor sperm IUI in India
- Fibroid uterus in India
- Myomectomy in India
- Laparoscopy in India
- Laparoscopy for Fallopian tube testing in India
- Advanced Laparoscopy in infertility in India
- Diagnostic Laparoscopy in infertility in India
- Hydrosalpinx treatment in India
- Laparoscopy for Hydrosalpinx in India
- Hydrosalpinx in infertility in India
- Laparoscopy for unexplained infertility in India
- Laparoscopy for endometriosis in India
- Endometriotic cyst removal in India
- ovarian cyst in India
- Laparoscopic cyst removal in India
- Hydrosalpinx tubal clipping in India
- Hydrosalpinx salpingectomy in India
- ovarian drilling in India
- laparoscopic ovarian drilling in India
- Hysteroscopy in infertility in India
- pre- IVF Hysteroscopy in India
- Diagnostic Hysteroscopy in India
- Operative Hysteroscopy in India
- Adhesiolysis Hysteroscopy in India
- synechiolysis in Hysteroscopy in India
- synechiae in India
- PGT in India
- Embryo freezing in India
- Frozen Embryo transfer in India
- Fresh embryo transfer in India
- Day 3 embryo transfer in India
- Assissted laser hatching in IVF in India
- Laser hatching in embryo transfer in India
- Blocked Fallopian tubes in India
- egg freezing in India
- embryo freezing in India
- Antagoist protocol in IVF in India
- Long protocol in IVF in India
- Dual stimulation in IVF in India
- Laparoscopy hysterectomy in India
- uterus removal in India
- laparoscopic uterus removal in India
- adenomyomectomy in India
- Adenomyoma in IVF in India
- Mirena insertion in India
- Irregular periods in India
- abnormal uterine bleeding in India
- dysfunctional uterine bleeding in India
- Normal Delivery in India
- Low Cost Delivery in India
- Caesarian in India
- LSCS in India
- Low cost LSCS in India
- Low cost caesarian in India
- Treatment of recurrent abortion in India
- repeated abortion in India
- Thin Endometrium in India
- asherman’s syndrome in India
- ERA in India
- endometrial receptive array in India
- Best ivf centre in Saket
- TESE in saket
- Laparoscopic cyst removal in saket
- ivf centre in South Delhi
- IVF Centre in South Delhi
- Infertility treatment in South Delhi
- IUI Centre in South Delhi
- IVF + ICSI centre in South Delhi
- Low cost IVF in South Delhi
- ovulation Induction in South Delhi
- Embryo transfer in South Delhi
- Blastocyst Transfer in South Delhi
- Female infertility treatment in South Delhi
- Male infertility treatment in South Delhi
- PCOS treatment in South Delhi
- PCOD treatment in South Delhi
- Polycystic ovaries treatment in South Delhi
- Endometriosis in South Delhi
- Endometrial Polyp in South Delhi
- Hysteroscopy Polypectomy in South Delhi
- Hysteroscopy septum resection in Saket
- Recurrent Implantation Failure treatment in South Delhi
- Repeated IVF Failure treatment in South Delhi
- PGD in South Delhi
- PGS in South Delhi
- Oncofertility treatment in South Delhi
- Best infertility Doctor in South Delhi
- Best IVF results in South Delhi
- Best IVF success rate in South Delhi
- Best IUI results in South Delhi
- Best IUI success rate in South Delhi
- Best ICSI centre in South Delhi
- Low cost IUI in South Delhi
- clomiphene citrate in South Delhi Letrozole in South Delhi
- Donor egg cycle in South Delhi
- Donor IVF in South Delhi
- Low sperm count in South Delhi
- Azoospermia in South Delhi Treatment of Azoospermia in South Delhi
- Testicular sperm extraction in South Delhi
- micro testicular sperm extraction in South Delhi
- TESA in South Delhi
- TESE in South Delhi
- PESA in South Delhi
- Microtese in South Delhi
- surgical sperm retrieval in South Delhi
- Donor sperm IUI in South Delhi
- Fibroid uterus in South Delhi
- Myomectomy in South Delhi
- Laparoscopy in South Delhi
- Laparoscopy for Fallopian tube testing in South Delhi
- Advanced Laparoscopy in infertility in South Delhi
- Diagnostic Laparoscopy in infertility in South Delhi
- Hydrosalpinx treatment in South Delhi
- Laparoscopy for Hydrosalpinx in South Delhi
- Hydrosalpinx in infertility in South Delhi
- Laparoscopy for unexplained infertility in South Delhi
- Laparoscopy for endometriosis in South Delhi
- Endometriotic cyst removal in South Delhi
- ovarian cyst in South Delhi
- Laparoscopic cyst removal in South Delhi
- Hydrosalpinx tubal clipping in South Delhi
- Hydrosalpinx salpingectomy in South Delhi
- ovarian drilling in South Delhi
- laparoscopic ovarian drilling in South Delhi
- Hysteroscopy in infertility in South Delhi
- pre- IVF Hysteroscopy in South Delhi
- Diagnostic Hysteroscopy in South Delhi
- Operative Hysteroscopy in South Delhi
- Adhesiolysis Hysteroscopy in South Delhi
- synechiolysis in Hysteroscopy in South Delhi
- synechiae in South Delhi
- PGT in South Delhi
- Embryo freezing in South Delhi
- Frozen Embryo transfer in South Delhi
- Fresh embryo transfer in South Delhi
- Day 3 embryo transfer in South Delhi
- Assissted laser hatching in IVF in South Delhi
- Laser hatching in embryo transfer in South Delhi
- Blocked Fallopian tubes in South Delhi
- egg freezing in South Delhi
- embryo freezing in South Delhi
- Antagoist protocol in IVF in South Delhi
- Long protocol in IVF in South Delhi
- Dual stimulation in IVF in South Delhi
- Laparoscopy hysterectomy in South Delhi
- uterus removal in South Delhi
- laparoscopic uterus removal in South Delhi
- adenomyomectomy in South Delhi
- Adenomyoma in IVF in South Delhi
- Mirena insertion in South Delhi
- Irregular periods in South Delhi
- abnormal uterine bleeding in South Delhi
- dysfunctional uterine bleeding in South Delhi
- Normal Delivery in South Delhi
- Low Cost Delivery in South Delhi
- Caesarian in South Delhi
- LSCS in South Delhi
- Low cost LSCS in South Delhi
- Low cost caesarian in South Delhi
- Treatment of recurrent abortion in South Delhi
- repeated abortion in South Delhi
- Thin Endometrium in south Delhi
- asherman’s syndrome in south Delhi
- ERA in south Delhi
- endometrial receptive array in south Delhi
- show more
- show less




